Attention: ENT physicians, audiologists, and hospitals
Please note that both Advanced Bionics and Med-EL are in-network durable medical equipment providers. They can provide in-network supplies and replacement parts for their branded cochlear implants for all of our members. Cochlear Americas is not currently an in-network provider.
When you prescribe cochlear implants made by an in-network vendor, the member will find it easier and more cost-effective to obtain replacement parts. As always, be sure to check eligibility and benefits before rendering services.
| Provider: | Phone |
|---|---|
| Advanced Bionics | 1-877-829-0026 |
| MED-EL Corporation | 1-888-633-3524 |
MPC_040918-1C-2-ART
This article is for all providers except dentists caring for our members
The American Medical Association (AMA) has released a series of dedicated telehealth evaluation and management codes effective January 1, 2025, as listed below. We will not be reimbursing these codes upon release. This decision aligns with the Centers for Medicare and Medicaid Services (CMS).
- 98000-98007: New or established patient audio-video codes
- 98008-98015: New or established patient audio only codes
Please continue to follow the guidelines in our Telehealth (Telemedicine) - Medical Services and Telehealth (Telemedicine) - Mental Health payment policies. We may reconsider reimbursing these new codes in the future and will communicate any updates as needed.
Related payment policies
Related payment policies
- Telehealth (Telemedicine) – Medical Services
- Telehealth (Telemedicine) – Mental Health
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or log in and go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_121624-3Q-1-ART
This article is for professional and facility providers who administer anesthesia
Blue Cross reimburses for anesthesia services as outlined in our existing Anesthesia payment policy().
As a reminder, there are several statements in the policy that describe how we pay claims. These include (but are not limited to):
- When anesthesia services are provided for multiple surgical procedures, only report the anesthesia code for the most complex service (with the highest base value) with the total time for all procedures performed.
- Blue Cross does not reimburse an E/M visit on the same day, the day before, or one day after the reporting of an anesthesia service.
- Blue Cross reimburses general anesthesia performed by the anesthesia provider, or under the anesthesiologist’s medical direction, at a rate not to exceed 100 percent of the anesthesia service allowable amount.
- Blue Cross does not recognize the use of revenue code 964.
Payment policy application
- Enforcement of this payment policy occurs through system edits and post-payment reviews.
- We continually expand our ability to process claims in accordance with this policy pre-payment, which will reduce the number of claims we review post-payment.
Important billing reminders
- Bill all anesthesia codes with the appropriate revenue code according to our policy.
- Bill multiple anesthesia services on a single line using the code with the highest base rate. List the total units for all anesthesia services.
- Blue Cross does not reimburse more than 100 percent of the allowed amount for the service.
Resources
Anesthesia payment policy (see the policy for additional billing guidelines). To download this payment policy, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
MPC_060921-2L-1
This article is for behavioral health practitioners
As a follow-up to us posting the September 1, 2020 professional fee schedule updates, we wanted to share a few reminders.
Blue Cross is still operating under the COVID-19 Temporary Payment Policy. As you know, we are currently reimbursing telehealth visits at the same rate as in-office visits. Please refer to this payment policy for specific reimbursement information for telehealth services.
Also, as noted in our July 23, 2020 press release, we will continue to reimburse behavioral health telehealth visits at the same rate as in-office visits even after the COVID-19 public health emergency ends. We will also update our payment policies accordingly once the public health emergency ends.
Resources
COVID-19 Information page
![]() COVID-19 Temporary Payment Policy
COVID-19 Temporary Payment Policy
![]() COVID-19 Temporary Professional Commercial and FEP Fee Schedule (log in and click Office Resources>Billing & Reimbursement>Fee Schedules)
COVID-19 Temporary Professional Commercial and FEP Fee Schedule (log in and click Office Resources>Billing & Reimbursement>Fee Schedules)
Questions?
Call Network Management and Credentialing Services at 1-800-316-BLUE (2583).
As always, thank you for the care you provide to our members.
MPC_030420-2D-2
Please share with your billing department or billing agency
We’re reminding providers about coordinating benefits and billing practices for your patients identifying as American Indian or Alaska Native (American Indians) who are enrolled in:
- A Blue Cross health plan; and
- An Indian Health Service (IHS) and tribal health Purchased/Referred Care (PRC) Program
Some providers are incorrectly billing a tribal health Purchased/Referred Care Program before billing the primary insurance for the member. This causes delays in payments to you and stress for the member.
Bill the primary insurer first
If a member is receiving medical or dental services from you and mention that they have “tribal insurance” please:
- Ask if they have other insurance
- If they do, make sure that your systems list their health insurance as primary.
- Bill their health insurance first
Indian Health Service and tribal health programs, including Wampanoag Health Service, help tribal members with their health needs, but are not health insurance plans. Federal rules require the Indian Health Service to be the payer of last resort for services provided to eligible persons.
Thank you for your help.
MPC_031023-2P-1
The Patient Protection and Affordable Care Act (ACA) requires all health plans, except grandfathered plans, to provide coverage for certain preventive care services at no additional cost.
 Our Patient Protection and Affordable Care Act Preventive Care Services Billing Guideline gives coding information about the ACA services that are available to our members. We’ve recently updated this document to reflect recent code and other changes.
Our Patient Protection and Affordable Care Act Preventive Care Services Billing Guideline gives coding information about the ACA services that are available to our members. We’ve recently updated this document to reflect recent code and other changes.
The ACA-required preventive services included are based on recommendations from the Advisory Committee on Immunization Practices, the U.S. Preventive Services Task Force, Bright Futures, the American Academy of Pediatrics, and the U.S. Department of Health and Human Services, including Women’s Preventive Health Services.
Services available at no cost
When provided by in-network providers, members do not pay additional costs for the services listed in our guideline document.
However, members with plans that include out-of-network or a self-referred level of benefits (for example, PPO and Blue Choice plans) will pay a cost share when these services are received from an out-of-network provider. In addition, some members' plans may be exempt from the ACA requirement.
As always, before performing services, please check the member’s eligibility and benefits.
MPC_071318-4C-5
This article is for providers discussing HIV PrEP with their patients
Please share with your billing
department or billing agency
We have updated our Patient Protection and Affordable Care Act preventive care services billing guideline to reflect the latest ICD-10-CM diagnosis code (Z29.81) for encounters related to HIV pre-exposure prophylaxis (PrEP). Please refer to page 4. This is in effect for dates of service on and after October 1, 2023.
How does this affect our members, your patients?
When a preventive care visit includes discussion of HIV PrEP, the member may be eligible for this preventive care service at no additional cost as part of the Patient Protection and Affordable Care Act (ACA).
The diagnosis code should be billed in the primary position on the claim since our benefits for preventive, screening, counseling, or wellness services are based on the primary diagnosis. Taking this step helps avoid unnecessary claim denials and confusion for our members, so we suggest sharing this information with your billing department.
Thank you.
As always, before performing services, please check the member’s eligibility and benefits.
MPC_071318-4C-9-ART
This article is for providers who care for our Medicare Advantage members
People who are enrolled in both Medicare and Medicaid—often called “dual eligibles”—meet Medicaid financial eligibility rules and also qualify for Medicare due to age, chronic illness, physical disability, mental health problems, or developmental disability.
Dual eligibles may receive assistance with Medicare cost-sharing from a State Medicaid program like MassHealth.
According to CMS rules, you cannot refuse to serve our Medicare Advantage members who are dually eligible. Here is some important information about billing when you provide services to dually eligible members.
| If you participate in our Medicare Advantage network and | Then when you provide services to dually eligible members |
|---|---|
| Accept Medicaid | You must:
|
| Do not accept Medicaid | You can collect deductible, co-insurance, or copayment amounts only if you notify the member and have them sign a non-covered service waiver form on the date of service* before you render services. |
*This ensures that the member understands that the form, a contract, allows you to collect fees for cost sharing.
Thank you
As always, thank you for the care you provide to your patients—our members.
MPC_112723-3Y
This article is for providers who bill for drugs and biologicals
As a reminder, our existing Drug Wastage payment policy applies to contracted providers who bill for covered, medically necessary drugs or biologicals.
As a reminder, our existing Drug Wastage payment policy applies to contracted providers who bill for covered, medically necessary drugs or biologicals. To access this fee schedule, login and go to Office Resources > Policies & Guidelines > Payment Policies.
Below are important billing guidelines outlined within our Drug Wastage payment policy. Please adhere to our payment policy to avoid a claim denial or post-payment recovery.
- Bill modifier JW for the drug amount discarded or not administered to any patient. The units billed must reflect the amount of discarded drug or biological and should be billed on a separate line from the amount of drug or biological administered, including Not Otherwise Classified (NOC) and unlisted codes.
- Units billed must be the appropriate size vial, or combination of vials, to deliver the appropriate administered dose.
- Submit the appropriate 11-digit National Drug Code (NDC) number used for any prescribed drug or biological administered for the date of service billed (including NOC and unlisted codes).
- Do not include hyphens when entering the NDC number.
- Also include any applicable revenue, HCPCS, and CPT codes.
- Document the reason for wastage in the patient’s medical record.
- Do not bill Blue Cross for:
- Drugs or biologicals that were not administered to the patient.
- Drug wastage associated with multi-use vial drugs or biologicals.
Please refer to our Drug Wastage payment policy for additional reimbursement and billing requirements.
Related payment policies
Questions?
If you have any questions, please call Network Management and Credentialing Services at
1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_061824-1P-1
This article is for obstetric providers and primary care providers caring for our members
As a reminder, we align with FDA recommendations and reimburse for the Respiratory Syncytial Virus (RSV) vaccine both for members aged 60+ and pregnant women within 32 to 36 weeks gestation.
When billing for the vaccine for pregnant women, please report the appropriate gestational week diagnosis on the claim to ensure accurate claim processing.
| RSV vaccine code | |
|---|---|
| 90678 | Respiratory syncytial virus vaccine, preF, subunit, bivalent, for intramuscular use |
| Gestational week diagnosis codes | |
| Z3A.32 | 32 weeks gestation of pregnancy |
| Z3A.33 | 33 weeks gestation of pregnancy |
| Z3A.34 | 34 weeks gestation of pregnancy |
| Z3A.35 | 35 weeks gestation of pregnancy |
| Z3A.36 | 36 weeks gestation of pregnancy |
Resources
- Immunizations payment policy
- Obstetrical and Maternity care payment policy
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines> Payment Policies.
MPC_011624-1L-1
This article is for all providers caring for Federal Employee Program members, including, but not limited to:
- Acute care hospitals discharging maternity patients postpartum
- Freestanding clinical laboratories
- Ground ambulance providers
- Lactation counselors

We’re noticing a trend in denied claims, leading to an increase in appeals for Federal Employee Program (FEP) members.
Below, you’ll find steps you can take to help your claims process smoothly for the topics listed. We hope this reduces your administrative time spent on claim appeals and decreases confusion for members about their coverage and health care costs.
Remember, you can recognize an FEP member by the “R” prefix, followed by eight digits, on their member ID card.
What’s the trend? Providers are submitting replacement claims without submitting a fully corrected claim. We’re seeing replacement claims submitted with only the newly corrected codes that weren’t on the original claim. All of the other information that was on the original claim that is correct is missing. This causes us to process the claim with the new information only, which isn’t always your intent.
What can you do?
- Be sure your replacement claim includes all codes for the date of service you’re billing us for. Please remember that by submitting a replacement claim, you are doing just that—replacing the complete claim. Therefore, all services should be included.
- Review our replacement claim resources.
What’s the trend? We’re seeing an increase in split billing and claims that don’t match the approved authorization. In some cases, labs are getting multiple prior authorizations for the same date and same service and submitting multiple claims.
What can you do?
- All services rendered by the same provider on the same date of service should be submitted on a single claim.
- Review the authorization approval for the service and make sure it matches the claim.
What’s the trend? Blue Cross Blue Shield of Massachusetts is receiving ground ambulance claims that should have been sent to the state where the service was rendered. Transport claims are also missing correct modifiers.
What can you do?
- Submit claims with appropriate modifiers for pick-up and drop-off locations. Refer to our Ambulance Transportation payment policy for a list.
- Submit claims with appropriate modifiers for pick-up and drop-off locations. Refer to our Ambulance Transportation payment policy for a list. Log in and go to Office Resources>Policies & Guidelines>Payment Policies.
- Send your claim to the Blue Cross Blue Shield plan of the state where services were rendered and where the member was picked up for transport. For example, if the FEP member is picked up in Rhode Island and is taken to a Massachusetts facility, you should submit the claim to Blue Cross Blue Shield of Rhode Island.
What’s the trend? When postpartum members are discharged from the hospital, they are often referred to virtual lactation counseling services with providers that aren’t covered by their telehealth benefits. FEP members do not have benefits to receive lactation counseling via telehealth from providers in our network.
What can you do?
- Review FEP member coverage by visiting fepblue.org.
- Refer them to Teladoc Health®' or refer them for in-person visits from network providers, both of which are covered.
Thank you!
MPC_050625-2S-1-ART
This article is for community mental health centers and opioid treatment programs caring for our members
Please share with relevant office staff and billing agencies
To ensure that your claims are processed correctly and efficiently, we encourage you to review and share the following tips with your billing department and any billing agencies that you may work with.
All services must be billed on a CMS-1500 claim form and include the following:
- Group NPI listed in both the Billing Provider and Rendering Provider fields (do not list an individual provider’s NPI)
- Correct modifier showing the licensure level of the rendering clinician (see table below)
|
Modifier |
Licensure level |
|---|---|
|
AF |
Psychiatrist |
|
AH |
Psychologist |
|
AJ |
Licensed independent clinical social worker (LICSW) |
|
HA |
Child psychiatrist |
|
HE |
Psychiatric nurse practitioner (PNP) |
|
Psychiatric physician assistant (PPA) |
|
|
HI |
Licensed applied behavioral analyst (LABA) |
|
Modifier |
Licensure level |
|---|---|
|
HH |
Licensed alcohol and drug counselor-1 (LADC-1) |
|
HR |
Licensed marriage and family therapist (LMFT) |
|
HO |
Licensed mental health counselor (LMHC) |
|
TD |
Mental health clinical nurse specialist |
|
HK |
Therapeutic behavioral services |
Note: Licensure modifiers should not be used when billing intermediate levels of care, such as intensive outpatient programs, partial hospitalization programs, crisis stabilization, and methadone maintenance.
For other important billing guidelines, please refer to our Community Mental Health Centers payment policy.
For other important billing guidelines, please refer to our Community Mental Health Centers payment policy.
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or log in and go to Office Resources>Policies & Guidelines>Payment Policies.
MPC_022525-1Q-1-ART
This article is for acute care hospitals caring for our members
During the COVID-19 Federal Public Health Emergency (PHE), COVID-19 laboratory services were reimbursed separately when billed with an outpatient surgical procedure. Starting in Q4 2023, COVID-19 laboratory services will no longer be separately reimbursed when billed with an outpatient surgical procedure. We will include reimbursement for the laboratory services in the outpatient surgical service’s case rate. This update aligns with the expiration of the COVID-19 Federal PHE earlier this year and Blue Cross’ existing payment policy.
As a reminder, Blue Cross reimburses outpatient surgical services at a case rate, which reflects the fee for each allowable surgery, including laboratory services directly related to the surgery. Refer to our Outpatient Surgical Services – Facility payment policy for additional information. To download this policy, log in and go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please contact Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_100223-1Y-1
This article is for all providers caring for our members
We recently updated our COVID-19 temporary payment policy with the following changes:
- Added new vaccine administrative code 90480.
- Added new vaccine codes 91318-91322.
- Indicated that vaccine code 91304 will be reimbursed by Blue Cross effective October 3, 2023 since it is no longer supplied for free from the state.
- Indicated deleted vaccine codes and vaccine administrative codes as of November 1, 2023.
| Code | Description | Reimbursed by Blue Cross effective date |
|---|---|---|
|
90480 |
Vaccine Administration SARSCOV2 VACC 1 DOSE |
September 11, 2023 |
|
91318 |
Pfizer-BioNTech COVID-19 Vaccine 2023-2024 Formula (Yellow Cap) |
September 11, 2023 |
|
91319 |
Pfizer-BioNTech COVID-19 Vaccine 2023-2024 Formula (Blue Cap) |
September 11, 2023 |
|
91320 |
Pfizer-BioNTech COVID-19 COMIRNATY (COVID-19 Vaccine, mRNA) 2023-2024 Formula |
September 11, 2023 |
|
91321 |
Moderna COVID-19 Vaccine 2023-2024 Formula |
September 11, 2023 |
|
91322 |
Moderna COVID-19 SPIKEVAX 2023-2024 Formula |
September 11, 2023 |
|
91304 |
Novavax Covid-19 Vaccine, Adjuvanted (Aged 12 years and older) |
October 3, 2023 |
Please see our COVID-19 temporary payment policy and applicable temporary COVID-19 fee schedules for additional information.
MPC_030620-1N-242-ART
This article applies to acute care hospitals and most professional providers but not these ancillary and behavioral health specialties.
We have updated our Temporary COVID-19 Professional Commercial and FEP Fee Schedule During COVID-19 Public Health Emergency.
To access the fee schedule updates, log in and go to Office Resources>Billing & Reimbursement>Fee Schedules.
Hospital Temporary COVID-19 fee schedule updates
- Please contact your network representative for the updated hospital outpatient fee schedule.
MPC_030620-1N-205
This article is for providers who bill for COVID-19 testing
| If patient is | Please use | Definition |
|---|---|---|
| Asymptomatic and without known COVID-19 contact |
|
|
|
Symptomatic or has been exposed to COVID-19 |
|
|
|
|
Example: The patient presents to the clinic for pre-surgical COVID-19 testing, has no symptoms, and no known contact. In this situation, use code Z11.59.
Questions?
Call Network Management and Credentialing Services at 1-800-316-BLUE (2583).
Resources
![]() COVID-19 temporary payment policy
COVID-19 temporary payment policy
MPC_030620-1N-129
This article is for physical therapists and occupational therapists caring for our members
We recently updated our Telehealth (Telemedicine) – Medical payment policy and Telehealth (Telemedicine) – Mental Health payment policy to allow procedure code 97535 to be reimbursable via telehealth effective October 27, 2023.
| Procedure code | Description | Telehealth reimbursement effective date |
|---|---|---|
| 97535 | Self-care/home management training (e.g., activities of daily living [ADL] and compensatory training, meal preparation, safety procedures, and instructions in use of assistive technology devices/adaptive equipment) direct one-on-one contact, each 15 minutes | October 27, 2023 |
Resources
For additional reimbursement information, please see our payment policies:
- Telehealth (Telemedicine) – Medical Services
- Telehealth (Telemedicine) – Mental Health
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_102323-1X-1
This article is for physicians and practitioners and their office staff and billing agencies
- Receive useful data insights about your claims
- Maximize coding efficiency and accuracy
- Reduce the burden of a traditional audit
It's well known that coding of Evaluation and Management (E/M) services is a challenge for many providers because it requires you to determine which level of CPT code appropriately reflects the complexity of the visit. More mistakes are made coding E/M services compared to coding for other services.
To help educate and inform practices on your E/M billing, we’re implementing Change Healthcare’s Coding Advisor solution (Coding Advisor) starting in September.
This is an educational program we’re offering to support your practice. It is not intended to question your treatment methods or clinical judgment.
What’s Coding Advisor and what will my practice receive?
Coding Advisor will review the use of billing for certain services for all providers submitting claims to Blue Cross. These may include, but are not limited to:
- Chiropractic services
- Complex services
- E/M codes
- Psychotherapy assessments
- Modifier 25 billing
Coding Advisor will contact qualifying providers on behalf of Blue Cross with a series of communications which may include:
- Mailed letters with reports for you to review your claim activity
- Educational phone calls from Coding Advisor’s mastery level professional coders
- Claim status messaging through the Change Healthcare Clearinghouse (when applicable).
Through this program, Coding Advisor will monitor billing practices and will send updated report(s) periodically. They may contact your practice to identify coding discrepancies and to provide customized coding education.
Contacting Coding Advisor
If you have questions, please call Coding Advisor Customer Support at
1-844-592-7009, Option 3.
Thank you in advance for taking the time to review and act on the information that Coding Advisor sends you.
MPC_123019-2J-1
When submitting either paper or electronic claims, please be sure to enter the member’s name exactly as it appears on their Blue Cross ID card. If you use nicknames, middle names, abbreviations, etc. that are not listed on their ID card, your claim(s) may result in a denial.
Examples
|
If the member’s ID card lists their name as |
But they prefer to be called |
You must still submit your claims with |
|---|---|---|
|
Robert |
Bob |
Robert |
|
Mary-Anne |
Maryanne |
Mary-Anne |
|
Sue Ellen |
Sue |
Sue Ellen |
|
Joseph Jr. |
Joe |
Joseph Jr. |
We appreciate your support in ensuring that your claims are processed correctly. And as always, thank you for the care you provide to our members.
MPC_010825-2G-1-ART
This article is for acute care hospitals caring for our Medicare Advantage members who are paid at the Medicare standard rate
In alignment with CMS and the CARES Act, relative weights for inpatient hospital claims for Medicare Advantage members diagnosed with COVID-19 are increased by 20 percent during the COVID-19 Public Health Emergency.
We would like to remind you that for dates of service on and after September 1, 2020, the patient’s medical record must include a positive COVID-19 laboratory test to qualify for this increase.
We may retroactively audit claims to ensure that Medicare Advantage claims with a COVID-19 diagnosis include a positive test.
MPC_030620-1N-131
This article is for all providers caring for our members
As you know, Blue Cross reimburses NOC (not otherwise classified) or unlisted CPT and HCPCs codes only when submitted with supporting documentation. In September 2024, we will clarify our General Coding and Billing payment policy regarding supporting documentation requirements. This update will allow for a more efficient, timely, and accurate review of claims billed with NOC codes.
For electronic claims, you may submit an appeal with supporting documentation. For paper claims, you may either submit the documentation with the claim itself, or in a separate appeal.
Payment policy application
Because unlisted codes do not describe a specific procedure or service, supporting documentation must contain clear, identifying information. This means that you should either circle or underline notes that identify the test or procedure associated with the unlisted code. The notes should be legible and contain the minimum necessary information to support the NOC code.
Note: We will only review clearly marked (circled,
underlined, etc.) notes.
You should already be following the guidelines below for NOC code supporting documentation. In September, we will include these criteria in our payment policy:
- A clear description of the type and extent of the procedure or service.
- Documentation should be specific to the procedure or service performed. Non-pertinent information should be omitted.
- Identify when the procedure was performed independently from other services provided, or if it was performed at the same surgical site or opening.
- Time, effort, and equipment necessary to provide the service, including any extenuating circumstances which may have complicated the service or procedure.
- The number of times the service was provided.
- When available, a similar or ‘treat-like’ code for the service represented by the NOC code.
- For drug NOC codes, NDC number is required.
If your supporting documentation does not adhere to these requirements, your claim’s processing will be impacted, with high potential for claim denial.
Resources
We will update our General Coding and Billing payment policy in September 2024 with these clarified guidelines.
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_051324-2X-1
This article is for cardiologists, endocrinologists, primary care providers, and their billing staff
Patients are excluded from the statin therapy quality measures if they:
- Are in hospice
- Are pregnant or breastfeeding
- Have cirrhosis
- Are being treated with in vitro fertilization (IVF)
- Have end stage renal disease (ESRD) or are being treated with dialysis
- Have myalgia, myositis, myopathy, or rhabdomyolysis diagnoses
Statin therapy quality measures assess patients diagnosed with diabetes or atherosclerotic cardiovascular disease (ASCVD) who receive and adhere to statin therapy. As you know, statin therapy can help prevent cardiovascular events, but some patients may not be clinically appropriate to receive statin therapy.
We review claims data to determine which patients to include or exclude from quality measures, based on their diagnosis. When you code your claims using the most current ICD-10-CM diagnosis code, we’ll automatically exclude ineligible patients from this quality measure.
The diagnosis code you use helps identify ineligible patients
Use the codes below to document patient conditions that prevent them from taking a statin.
| For patients with this condition | Use the appropriate code |
|---|---|
| Cirrhosis | K70.30, K70.31, K71.7, K74.3, K74.4, K74.5, K74.60, K74.69 |
| Dialysis procedure | G0257 |
| End stage renal disease | N18.6 |
| Hospice care | G9473-G9479 |
| IVF procedure | S4015, S4016, S4018, S4020, S4021 |
| Myalgia | M79.1-M79.18 |
| Myositis | M60.80-M60.819, M60.821-M60.829, M60.831-M60.839, M60.841-M60.849, M60.851-M60.859, M60.861-M60.869, M60.871-M60.879, M60.88-M60.9 |
| Myopathy | G72.0, G72.2, G72.9 |
| Rhabdomyolysis | M62.82 |
| Pregnancy | G9778 |
Please note that there are many codes that may exclude members from statin quality measures; the list above is a sample of diagnosis and procedure codes that may be used.
We also understand that there are patients with mild myalgias of unclear relationship to statins, and for whom statins are critical therapy. If you have worked through a careful continuation plan with your patient, they may also be excluded from the HEDIS quality measures.
Using these codes will exclude members from the HEDIS measure’s eligible population and help to determine possible gaps in care.
Thank you
As always, thank you for the care you provide to our members.
MPC_032122-2B-1
This article is for anesthesiologists and gastroenterologists caring for our members
As we’ve previously notified and reminded you, effective January 1, 2024, we will implement diagnosis-driven claim edits to reinforce our existing monitored anesthesia care (MAC) medical policy 154 guidelines.
For our enforcement of this policy on January 1, 2024, it’s important to know that we cover monitored anesthesia care for endoscopic procedures such as colonoscopies and upper endoscopies when medically necessary. Medical policy 154 lists diagnosis codes and clinical scenarios where monitored anesthesia care is medically necessary for endoscopic procedures, outlined by certain medical conditions and complication risks.
Our medical policy aligns with the American Society of Gastrointestinal Endoscopy (ASGE), American College of Gastroenterology, American Gastroenterological Association, and American Society of Anesthesiologists (ASA) guidelines.
Why are we implementing this enforcement?
- In accordance with the above guidelines, endoscopic procedures can be performed under either moderate sedation or monitored anesthesia care.
- In appropriately selected patients, moderate sedation is comparably safe and more cost effective than monitored anesthesia care.
- The member’s cost share is the same for either monitored anesthesia care or moderate sedation, and the amount is based on their plan benefits.
- Note: If an endoscopic procedure is performed under monitored anesthesia care and does not align with medical policy 154, the member is not liable for the non-covered amount.
As a result of processing claims in accordance with our policy on a pre-payment basis, we are able to reduce the number of claims needing post-payment review.
Resources:
- Medical policy 154 - Monitored Anesthesia Care (MAC)
- May 19 news article: We are postponing our monitored anesthesia care claim edits
- August 1 news article: Reminder for January 1 monitored anesthesia care claim edits
MPC_120522-1Q-6-ART
This article is for all providers caring for our members
As you know, many provisions of the Consolidated Appropriations Act (CAA) of 2021 and the Transparency in Coverage Final Rule began impacting our members starting Jan. 1, 2022. As providers caring for our members, some of these provisions may impact you as well.
Here are highlights of these federal requirements. We’ll continue to publish more information as it becomes available. We advise you to consult with your own legal advisors for information on the obligations that may apply to your practice.
Provider directory (plan years beginning on or after Jan. 1, 2022)
CAA requires provider directory information to be verified every 90 days. Providers and health insurers have roles in fulfilling this requirement to maintain an accurate directory for members. Read more on the new requirements.Machine-readable files
Health insurers are required to publicly display certain health care price information via machine-readable files on their websites beginning July 1, 2022. These machine-readable files will include negotiated rates with in-network providers, allowed amounts for out-of-network providers and may include prescription-drug pricing.
Member ID cards (plan years beginning on or after Jan. 1, 2022)
The CAA requires that member ID cards include deductible information and out-of-pocket maximums. Starting in the 2nd quarter of 2022, we will begin re-issuing cards in the new format. Members’ current cards remain valid for all services. and member ID numbers will not change. Members who have questions about their new ID card can contact the Member Services 1-800 on the back of their card.
Continuity of Care (plan years beginning on or after Jan. 1, 2022)
Most of our group and fully insured plans include a period of continuity of care at in-network reimbursement rates when a provider leaves our networks. Continuity of care applies to members who are undergoing active treatment for a serious or complex condition, pregnant, or a terminal illness. The CAA requires up to 90 days of continued, in-network care for affected members when:
- A provider’s network status changes (note that this does not include for-cause terminations)
- A group health plan changes health insurance issuer, resulting in the member no longer having access to a participating provider in our network.
For members who qualify for continuity of care, you will need to accept payment at the in-network rate.
No Surprises Act (beginning on Jan. 1, 2022)
Under the No Surprises Act, most out-of-network providers will no longer be allowed to balance bill patients for the difference between the provider's charge and the allowed amount for:
- Emergency services (learn about the updated definition of emergency services)
- Out-of-network care during a visit to an in-network facility
- Out-of-network air ambulance services, if patients’ benefit plan covers in-network air ambulance services.
Gag Clauses (effective Dec. 27, 2020)
CAA prohibits health insurers and group health plans from entering into provider agreements that include gag clauses related to provider cost and quality information. If any of our provider contracts include language that contradicts the CAA gag clause requirement, the contract language will be remediated, and in the interim, the language will be considered unenforceable as a matter of law.
MPC_120921-1H-1
This article is for durable medical equipment suppliers.
Blue Cross covers continuous passive motion devices as described in Continuous Passive Motion in the Home Setting Medical Policy 407.
As a reminder, the medical policy describes conditions that must be met for the device to be covered for our commercial and Medicare Advantage members.
Payment policy application
- Enforcement of this medical policy occurs through system edits and post-payment reviews.
- We continually expand our ability to process claims in accordance with this policy pre-payment, which will reduce the number of claims we review post-payment.
Resources
The included codes and diagnoses are listed in the medical policy, which will be updated on our website on April 1.
MPC_020922-3E-1
This article is for dentists and oral surgeons caring for our members
To make sure that we process your coordination of benefits electronic submissions correctly, please check whether you are using the most up-to-date version of your practice management software and that it can support line-level data entry.
Before submitting claims electronically, you must determine the primary payer and submit the claim to that payer first. When Blue Cross and Blue Shield of Massachusetts is the secondary payer, you must report:
- the primary insurer’s name and address
- the insured member’s ID number for that insurer
- for claims paid by the other insurer*, report the amount paid at the claim’s line level. We recommend contacting your practice management software vendor to ensure each claim line being reported has either the primary insurance paid amount or reject reason. Your claim may be rejected if this data is not supplied.
- for claims that were denied by the primary insurer, report the reject reason.
*You can learn more on our dedicated coordination of benefits page, including a member fact sheet.
MPC_030222-3R-12-ART
This article is for durable medical equipment providers caring for our members
We’d like to remind you that effective June 1, 2022, we’ll require prior authorization for power wheelchairs and continuous glucose monitors (CGM).
Power wheelchair authorization requirements
As you may recall, we’ll require authorization for power wheelchairs for our commercial and Medicare Advantage members. We informed you in December 2021 of upcoming changes to medical policy 365: Manual and Power Operated Wheelchairs.
Please note that these prior authorization requirements only apply to the codes listed below. Other equipment listed in the medical policy, such as accessories and manual wheelchairs, don’t require prior authorization.
Power wheelchair HCPCS codes requiring prior authorization
When submitting requests for prior authorization, only submit the appropriate power wheelchair code along with supporting clinical documentation.
| K0813 | K0825 | K0837 | K0850 | K0859 |
| K0814 | K0826 | K0838 | K0851 | K0860 |
| K0815 | K0827 | K0839 | K0852 | K0861 |
| K0816 | K0828 | K0840 | K0853 | K0862 |
| K0820 | K0829 | K0841 | K0854 | K0863 |
| K0821 | K0830 | K0842 | K0855 | K0864 |
| K0822 | K0831 | K0843 | K0856 | K0890 |
| K0823 | K0835 | K0848 | K0857 | K0891 |
| K0824 | K0836 | K0849 | K0858 | K0898 |
If you submit codes for services that don’t require prior authorization (for example, K0108), we won’t review them or notify you of any decision. We’ll continue to deny reimbursement for K0108 when billed. If medically necessary, please appeal with the clinical documentation to support the claim.
Continuous glucose monitors requiring prior authorization
We also wanted to remind you of our previous notification about expanding authorization requirements for continuous glucose monitors (Codes: A9277, K0553, S1036) to our commercial EPO and PPO members as of June 1.
Read our April 15 news article reminder.
Resources
- Manual and Power Operated Wheelchairs Medical Policy 365
- Durable Medical Equipment Payment Policy – Log in and go to Office Resources>Payment Policies.
- 2022 Fee schedule updates, reminders News Alert – Log in and go to News. Scroll to December 22, 2021 and look for the red exclamation point next to the News Alert titled, “2022 fee schedule updates, reminders."
MPC_052322-1P-1
This article is for providers who care for our Medicare Advantage members
People who are enrolled in both Medicare and Medicaid—often called “dual eligibles”—meet Medicaid financial eligibility rules and also qualify for Medicare due to age, chronic illness, physical disability, mental health problems, or developmental disability.
Dual eligibles may receive assistance with Medicare cost-sharing from a State Medicaid program like MassHealth.
According to CMS rules, you cannot refuse to serve our Medicare Advantage members who are dually eligible. Here is some important information about billing when you provide services to dually eligible members.
| If you participate in our Medicare Advantage network and | Then when you provide services to dually eligible members |
|---|---|
| Accept Medicaid | You must:
|
| Do not accept Medicaid | You can collect deductible, co-insurance, or copayment amounts only if you notify the member and have them sign a non-covered service waiver form on the date of service* before you render services. |
*This ensures that the member understands that the form, a contract, allows you to collect fees for cost sharing.
Thank you
As always, thank you for the care you provide to your patients—our members.
MPC_112723-3Y
This article is for all professional providers caring for our Medicare Advantage members
For Medicare Advantage members, we no longer accept professional 1500 claims that have a total charge greater than $99,999.99. This change aligns with the Centers for Medicare & Medicaid Services (CMS) billing guidelines and does not apply to commercial or Federal Employee Program (FEP) members.
If you submit a single, professional claim with charges greater than this amount, your claim will be denied. If you need to bill for services that have more than the allowed charges:
- Split your submission into multiple claims.
- Use modifier 76 on the subsequent claims to indicate that they are not duplicate.
- Ensure that your total charges are different on each claim.
Example
If your total charge is $100,000:
- Submit claim 1 with a total charge of $80,000 (or any amount under $99,999.99).
- Then, submit claim 2 with the remaining $20,000 and use modifier 76 to indicate that it is a repeat service.
As always, thank you for your understanding and for the care you provide to your patients, our members.
MPC_042925-1P-1
This article is for hospitals and physicians caring for our members
To ease the strain on busy emergency rooms, Blue Cross will reimburse out-of-network urgent care centers in eastern Massachusetts* for medically necessary services provided to our members** this summer.
This change will be in effect from July 3 to October 1, 2024. This is intended to comply with the Healey/Driscoll Administration’s Memorandum dated June 26, 2024—90-day Urgent Care Strategy to Address Emergency Department Capacity.
Urgent care providers may not balance bill
During this period, urgent care centers in eastern Massachusetts may not balance bill Blue Cross patients for medically necessary urgent care services.
How we are educating our members
We’re educating members about where they can find urgent care if they need it this summer.
*Eastern Massachusetts is defined to include the following counties: Essex, Middlesex, Suffolk, Norfolk, Bristol, Plymouth, Barnstable, Dukes, and Nantucket.
**Excludes Federal Employee Program members.
MPC_061724-1S-2
This article is for physicians, practitioners, their office staff and billing agencies
Please share with relevant office staff and billing agencies
How can the Billing Outlier Program support you?
- Receive useful data insights about your claims
- Maximize coding efficiency and accuracy
- Reduce the burden of a traditional audit
It's well known that coding of Evaluation and Management (E/M) services is a challenge because it requires determining the appropriate CPT code level that reflects the complexity of the visit. More mistakes are made coding E/M services than coding for other services.
To help inform practices on E/M billing, we’re implementing a new Billing Outlier Program starting in May. This educational program is designed to support coding decisions—not to question your treatment methods or clinical judgement.
What does the Billing Outlier Program entail?
Through this program, we will review billing for certain services for all provider-submitted claims, including but not limited to:
- Chiropractic services
- Complex services
- E/M codes
- Modifier 25 billing
- Psychotherapy assessments
To prepare, we will send a series of letters with reports of claims activity to qualifying providers. To provide further support, we’ll conduct reviews of your claim activity and send updated report(s) periodically.
Questions?
We know that many factors can affect how you bill, and we’re here to help you. If you have questions about this program, please call Provider Service at 1-800-882-2060.
This article is for all providers caring for our members
Effective July 18, 2022, we will enhance our claims editing system to improve its overall accuracy regarding modifier usage. Currently, some modifiers including, but not limited to, 25, 59 (X-EPSU subset), 79, and 24 are inappropriately overriding unbundling edits in certain situations. Based on an extensive assessment of modifier use, the Office of Inspector General (OIG) and the Centers for Medicare & Medicaid Services (CMS) have advised the use of pre-payment modifier review based on claim details and patient claim history.
Consistent with the recommendations of the OIG and CMS, Blue Cross will implement enhanced editing based on national guidelines for modifier usage. As part of this process, registered nurses with coding certifications will look at claim data in conjunction with patient claim history to confirm appropriate modifier use.
You can review guidelines for correct modifier use in:
- The Current Procedural Terminology (CPT) and Coding with Modifiers manuals, published by the American Medical Association
- The Correct Coding Initiative (CCI) and CMS claims processing manuals, published by the Centers for Medicare & Medicaid Services
Upon implementation of our enhanced editing system, you may submit an appeal with the appropriate medical records and documentation to support modifier use.
Questions?
If you have any questions, please call Network Management and Credentialing Services at
1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_041322-1S-1-ART
This article is for all providers caring for our members
In an effort to continue to increase access to mental health services for our members, we are pleased to announce an update to telehealth reimbursement. Effective for dates of service on or after August 1, 2022, when a claim includes a primary/principal diagnosis code only of F01 through F99 (indicating the primary nature of the visit is mental, behavioral, or neurodevelopmental disorders), we will reimburse telehealth at the same rate as in-person visits for all providers, regardless of specialty.
For additional information about reimbursement and billing guidelines, please refer to our Telehealth payment policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at
1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
Related payment policies
- Telehealth (Telemedicine) - Medical Services
- Telehealth (Telemedicine) - Mental Health
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Related payment policies
MPC_062822-2S-1-ART
Effective October 1, 2022, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
As always, thank you for the care you provide to your patients—our members.
Effective October 1, 2022, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_111521-4P-10-ART
This article is for acute care hospitals caring for our members
Effective October 1, 2023, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedulescommercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
This article is for acute care hospitals caring for our members
Effective October 1, 2024, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
As always, thank you for the care you provide to your patients—our members.
Effective October 1, 2024, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_101923-1P-7
Effective October 1, 2020, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_111819-4W-10
Effective October 1, 2021, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_113020-1K-10
We are aware that billing claims when the member has more than one insurer (requiring coordination of benefits) can be confusing, and that this confusion may cause claims to be denied or retroactively adjusted. We’d like to help you, your billing staff, and software vendors submit claims successfully.
Please take a few minutes to help us understand the root causes of these problems. Click on the link below for a brief survey:
This article is for psychiatrists, primary care providers, acute care hospitals, and community mental health centers caring for our members
Intravenous ketamine and intranasal esketamine share the same medical necessity criteria for treatment-resistant depression, found in our medical policy 087. For that reason, you can use an approval for one drug/procedure for either treatment during the approval period without requesting a new prior authorization. Here are some tips to help you request authorization and bill for services:
|
When you are |
Please |
|---|---|
|
Requesting authorizations for either intravenous ketamine or intranasal esketamine |
|
|
Billing for the service |
|
MPC072023-1F-1-ART
This article is for acute care hospitals caring for our members
As a reminder, our existing Inpatient Acute Medical Admission payment policy applies to contracted providers rendering covered, medically necessary inpatient care.
You must follow the below important billing guidelines for outpatient and observation services preceding an inpatient admission, as currently outlined in our payment policy.
|
For hospitals that are |
Follow these billing guidelines |
|---|---|
|
Reimbursed under APR-DRG methodology |
|
|
Not reimbursed under APR-DRG methodology |
|
Blue Cross reserves the right to perform post-payment review when services are not billed in accordance with our payment policies.
Related payment policies
To view payment policies, log in and go to Office Resources>Policies and Guidelines>Payment Policies.
- Ambulance Transportation
- General Coding and Billing
- Inpatient Acute Medical Admission
- Newborn and Neonatal Intensive Care Services
- Non-Reimbursable Services
- Observation Services
- Serious Reportable Events
- Third Party Services
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_041023-3U-1-ART
This article is for orthodontists and general dentists caring for our members
As we communicated to you in a November 5, 2021 News Alert, the CDT codes listed below for interceptive orthodontic treatment will be deleted from your fee schedule beginning January 1, 2022. This change was based on updates to the CDT 2022 code set from the American Dental Association (ADA). We’d like to remind you that we will deny any claims submitted with the following codes for dates of service on and after January 1, 2022:
Deleted CDT codes effective January 1, 2022

| CDT Code | Narrative |
|---|---|
| D8050 | Interceptive orthodontic treatment of the primary dentition |
| D8060 | Interceptive orthodontic treatment of the transitional dentition |
| D8690 | Orthodontic treatment (alternative billing to a contract fee) |
We are in the process of updating our CDT Procedure Guidelines and Submission Requirements for 2022 and will post it online before January 1. Please be sure to consult the orthodontic section of this manual for codes that may be billed for orthodontic care.
Resources
To read the November 5 News Alert, log in, go to News, and click the headline, "2022 Maximum Allowable Charge and Medicare Advantage enhancement."
Questions?
If you have any questions, please call Dental Network Management at 1-800-882-1178. As always, thank you for the care you provide to our members.
MPC_010821-1K-7
This article is for mental health providers caring for our members
Effective November 1, 2022, the following interprofessional telephone/internet/electronic health record assessment and management services will be reimbursable only to mental health professional and facility providers. This payment policy applies to all products, excluding FEP.
For acute care and mental health hospitals and facilities that bill on a UB-04 form, you must bill the below codes with professional mental health revenue code 961. There is no telehealth reimbursement for any facility overhead.
| Code | Description |
|---|---|
| 99446 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 5-10 minutes of medical consultative discussion and review |
| 99447 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 11-20 minutes of medical consultative discussion and review |
| 99448 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 21-30 minutes of medical consultative discussion and review |
| 99449 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 31 minutes or more of medical consultative discussion and review |
| 99451 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a written report to the patient's treating/requesting physician or other qualified health care professional, 5 minutes or more of medical consultative time |
| 99452 | Interprofessional telephone/internet/electronic health record referral service(s) provided by a treating/requesting physician or other qualified health care professional, 30 minutes |
Resources
![]() Mental Health and Substance Use payment policy
Mental Health and Substance Use payment policy
![]() Non-Reimbursable Services payment policy
Non-Reimbursable Services payment policy
![]() Telehealth (Telemedicine) - Mental health payment policy
Telehealth (Telemedicine) - Mental health payment policy
Resources
- Mental Health and Substance Use payment policy
- Non-Reimbursable Services payment policy
- Telehealth (Telemedicine) - Mental health payment policy
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_092822-1C-1
This article is for acute care hospitals, limited service clinics, physician offices, and urgent care centers caring for our members
We've noticed that claims for lab services sometimes omit the ordering clinician NPI. Please remember to include the ordering clinician NPI when billing for all lab services (including COVID-19 testing).
Be sure to complete loop 2310A (claim level) on the 837 Professional electronic claim form.
Or, if you need to submit your claim on paper, complete fields 17A & B on the CMS-1500 health insurance claim form, as shown below:

Inappropriate claims may be denied.
MPC_103020-1Y-1
This article is for acute care hospitals where our members receive outpatient surgery
Blue Cross reimburses for outpatient surgical services as outlined in our existing outpatient surgical services facility payment policy.
As a reminder, we reimburse outpatient surgical services at a case rate, which reflects the fee for each allowable surgery, including laboratory services related to the surgery.
The existing outpatient surgical services facility payment policy states that Blue Cross:
- Separately reimburses laboratory, radiology, or other diagnostic tests or procedures that are unrelated to the surgical procedure.
- Does not separately reimburse services, such as laboratory, that are related to the allowable surgical procedure. Reimbursement is included as part of the surgical case rate.
Payment policy application
- Enforcement of this payment policy will occur through post-payment reviews.
- In the third quarter of 2021, we will have the ability to process claims in accordance with this policy pre-payment, which will reduce the number of claims being reviewed post-payment.
Important billing reminders
- Bill all CPT and HCPCS codes with the appropriate revenue code to trigger the correct surgery case rate.
- Bill all facility services administered on the day of the surgery on the same claim form to ensure accurate reimbursement. Certain services should be billed on individual lines so they can be individually priced.
- Bill multiple surgeries on the same claim form with the appropriate revenue codes and corresponding valid CPT or HCPCS surgical procedure codes.
See payment policy for additional billing guidelines.
Questions?
Call Provider Service at 1-800-882-2060. As always, thank you for the care you provide to your patients—our members.
Resources
![]() Outpatient surgical services facility payment policy (log in and go to Office Resources>Policies & Guidelines>Payment Policies)
Outpatient surgical services facility payment policy (log in and go to Office Resources>Policies & Guidelines>Payment Policies)
MPC_022521-1E-1-ART
This article is for dentists and oral surgeons caring for our members
We now offer an online CDT look-up tool that can streamline the way you do business with us. By providing you with plan-specific procedure guidelines and submission requirements, it can save you time that you — or your billing agency — might spend calling us. And, it’s available any time of the day or night!
Want to learn more?
Watch our 3-minute video to learn to use the CDT lookup tool. The video and tool can both be found here.
MPC_011223-2K-5-ART
We’ve posted a link to the recorded webinar and answers to questions received during the presentation. Refer to the links below.
This article is for all providers (except dentists) caring for our members and their office staff
Join us for a claims overview webinar designed for all medical providers on Thursday, May 27, 2021 from noon – 1 p.m. Our Blue Cross experts will cover these topics and more, leaving time for questions:
- Walkthrough of the life cycle of a claim
- Verifying benefits/eligibility
- Submitting claims/replacement claims tips
- BlueCard (what it is and what makes it different)
- Tracking claim status and payments on Payspan
- Follow-up/appeal guidelines
- Provider Central overview
Before the presentation, we’ll post a copy of the slides here for your convenience.
Attending the webinar
Please register for the webinar using the link below so we know how many will attend. We’ll need attendee name and information about your practice or organization, such as NPI and specialty.
Additionally, you have the option of submitting questions through the registration survey. We’ll also take questions during the event, but submitting them in advance will help us determine the topics of focus. We will be collecting these until May 15.
How to join
- Paste this link into your web browser https://primetime.bluejeans.com/a2m/live-event/tbpepqps
- Under Join as Guest, enter your first and last name and email address. Select "Join As Guest." Then select "Join by browser."
Can't attend?
We'll update this news article with a recording of the webinar and answers to your questions about one week after the session.
Resources
![]() Quick Tip: Correcting Claim Rejections
Quick Tip: Correcting Claim Rejections
![]() Webinar slides
Webinar slides
![]() Answers to your questions (FAQ)
Answers to your questions (FAQ)
Recording of webinar
As always, thank you for the care you provide to your patients—our members.
MPC_040221-3B-2
This article is for providers caring for our Medicare Advantage members
We’d like to make you aware of upcoming cost share changes to Part B benefits that will happen this year as part of the Inflation Reduction Act. These changes apply to all of our Medicare Advantage plans.
- Starting April 1, 2023, Medicare Advantage members may pay a lower co-insurance for some Part B drugs if the drug’s price increased faster than the rate of inflation.
- Starting July 1, 2023, Medicare Advantage members taking insulin will not pay more than $35 for a month’s supply of insulin furnished under Part B. This limit only applies to the insulin itself, and not the pump or other durable medical equipment associated with Part B insulin.
What lower co-insurance means for you
If you collect co-insurance from a member on the date of service, and the member pays more than the adjusted co-insurance for a Part B rebatable drug, you may have to issue a refund to that member. Therefore, we strongly encourage you to bill the member after the claim has paid.
The Centers for Medicare & Medicaid Services (CMS) will publish the adjusted co-insurance for each Part B rebatable drug in the quarterly pricing files posted on the CMS website. Keep in mind the list of applicable drugs and members’ co-insurance for those drugs could change each quarter.
Some plans may also have co-insurance that is less than the co-insurance listed in these pricing files. In this scenario, members will pay the lower co-insurance.
Questions?
For more information on reduced drug prices, and enhanced Medicare benefits under the Inflation Reduction Act, refer to the CMS Frequently Asked Questions.
MPC_022123-1N
This article is for the acute hospitals, physicians, and ancillary providers caring for our members
As part of the Coronavirus Aid, Relief, and Economic Security (CARES) Act, the Centers for Medicare & Medicaid Services (CMS) has extended the suspension of the mandatory payment reductions known as “sequestration” through December 31, 2021. Beginning on January 1, 2022, sequestration will be reinstituted.
If you have any questions, please contact your network representative.
MPC_020620-1N-189-ART
This article is for all participating providers
The Protecting Medicare and American Farmers from Sequester Cuts Act will reinstate the Medicare payment adjustment known as “sequestration” effective April 1, 2022. From April 1, 2022 to June 30, 2022, the Centers for Medicare & Medicaid Services (CMS) will apply a 1% payment adjustment. Beginning July 1, 2022, CMS will apply a 2% payment adjustment.
Questions
If you have any questions, please contact your network representative.
MPC_030620-1N-228
This article is for all providers caring for our members
In response to the monkeypox public health emergency, we would like to provide guidelines on how to bill for the administration of the monkeypox vaccine.
- We do not reimburse monkeypox vaccine codes 90611 and 90622, as they are provided free from the state.
- We do reimburse the administration of the vaccine.
- Although we do not reimburse monkeypox vaccine codes, you still need to bill these codes along with the related administration codes on your claim.
As a reminder, modifier SL is used to indicate a non-reimbursed, state-supplied vaccine. The monkeypox vaccine will be accepted if billed with or without modifier SL. See our Immunization payment policy for additional guidelines.
As a reminder, modifier SL is used to indicate a non-reimbursed, state-supplied vaccine. The monkeypox vaccine will be accepted if billed with or without modifier SL. See our Immunization payment policy for additional guidelines. To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
To report vaccine administration, bill the existing vaccine administration codes (90460, 90461, 90471, 90472) according to the patient’s age and the administration(s) given during the visit.
| Code | Description | Comments |
|---|---|---|
| 90611 | Smallpox and monkeypox vaccine, attenuated vaccinia virus, live, non-replicating, preservative free, 0.5 mL dosage, suspension, for subcutaneous injection | Not reimbursed as the vaccine is provided free from the state |
| 90622 | Vaccinia (smallpox) virus vaccine, live, lyophilized, 0.3 mL dosage, for percutaneous use | |
| 90460 | Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care professional; first or only component of each vaccine or toxoid administered | Use to report the administration of 90611 or 90622 |
| 90461 | Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care professional; each additional vaccine or toxoid component administered (list separately in addition to code for primary procedure) | |
| 90471 | Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); 1 vaccine (single or combination vaccine/toxoid) | |
| 90472 | Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); each additional vaccine (single or combination vaccine/toxoid) (list separately in addition to code for primary procedure) |
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_083122-1E-1
This article is for the health care facilities that provide nasal naloxone to our members
As part of a Massachusetts law that takes effect on July 1, 2025, we’ll now offer members a new coverage option to receive a two-dose nasal naloxone pack using their medical benefits1.
Today, no-cost nasal naloxone packs are available without a prescription from retail pharmacies and are covered by our pharmacy benefits. Beginning July 1, you may dispense these two-dose packs to our members at the time of discharge or during a visit.
About our medical benefit coverage for nasal naloxone packs
- This applies to commercial and Medicare supplemental plans only (excludes Federal Employee Program plans and Medicare Advantage plans).
- There is no member cost share for most plans. Members who have a high-deductible plan may be responsible for the full cost of the pack unless they’ve already met their health plan deductible for the year2. (To help these members avoid a cost share, they can fill nasal naloxone packs at a pharmacy).
How to bill us for nasal naloxone packs
For dates on or after July 1, health care facilities distributing a two-dose pack of nasal naloxone* to our members using their medical benefits must bill Blue Cross as described below:
- Commercial members who do not have a high-deductible health plan will have a $0 cost share applied when you bill in this way. (You’ll see this on your provider detail advisory).
- If the member has a high-deductible plan, you will see any costs you can collect listed on the provider detail advisory.
- When Medicare is primary, continue to bill as you would to Medicare with applicable coding for nasal naloxone.
| When billing for nasal naloxone on a UB or 1500 claim | Use | With this modifier | And include |
|---|---|---|---|
| J3490 | HG |
|
* Naloxone nasal spray comes in a package containing two 4-mg doses of naloxone.
Blue Cross will reimburse the following providers for nasal naloxone packs
- Acute care hospitals
- Rehabilitation hospitals
- Mental health hospitals, mental health detox facilities and state psychiatric hospitals
- Community mental health centers
- Opioid treatment programs
Blue Cross will not reimburse
- Naloxone nasal spray packs received for free/not intended for resale.
Resources
- Fee schedules will be updated to comply with this Massachusetts Division of Insurance Filing Guidance 2025-F.
- General Coding and Billing payment policy will be updated to include these billing requirements on July 1, 2025.
- Massachusetts Division of Insurance Filing Guidance 2025-F.
- Providers can confirm the deductible amount and the amounts that have already been applied by checking the member’s benefits and eligibility online or by calling Provider Service.
MPC_032625-1M-2
This article is for billing and appeals staff at acute care facilities and surgical day care centers caring for our members
Equian, a nationally known payment integrity vendor, partners with us to review select inpatient facility claims before payment. We want to let you know about some changes that will take effect on June 1, 2023 to the addresses you use to submit necessary information for Equian to complete their pre-payment reviews.
Please see the grid below and make sure you notify any impacted departments or staff. Communications from Blue Cross Blue Shield of Massachusetts and Equian will be updated with the new contact information on June 1, 2023.
|
For Equian requests related to |
Continue to use this contact information | Begin using this new contact information as of June 1, 2023 |
|---|---|---|
| Itemized bill requests |
claimsadmin@equian.com Fax: 1-800-435-2049 |
New email to submit itemized bill requests: mca@equian.com |
| Reconsiderations/appeals |
reconsiderations@equian.com Fax: 1-866-700-5769 |
New mailing addresses for document submission:
USPS mail: UPS/FedEx packages: |
| Provider report |
reconsiderations@equian.com claimsresolution@equian.com |
|
| Resolutions |
claimsresolution@equian.com Phone: 1-800-806-9784 |
No change |
If you have any questions, please reach out to your Blue Cross Network Representative.
MPC_031323-2T-1
This article is for providers caring for our Medicare Advantage members
CMS has issued its final coverage criteria for pre-exposure prophylaxis (PrEP) for human immunodeficiency virus (HIV) prevention. Based on this guidance, members of our Medicare Advantage plans will have coverage, effective immediately, for the following:
- PrEP using antiretroviral drugs (whether oral or injectable) approved by the U.S. Food and Drug Administration (FDA) to prevent HIV infection in individuals at high risk of HIV acquisition.
- Up to eight individual counseling visits, every 12 months, that include HIV risk assessment (initial or continued assessment of risk), HIV risk reduction, and medication adherence.
- HIV screening up to eight times every 12 months and a single screening for hepatitis B virus (HBV) for individuals being assessed for, or who are taking, PrEP.
We will cover PrEP, the additional screening tests, and counseling services at a $0 cost-sharing preventive service when provided by an in-network provider.
Billing and payment codes for the other covered services related to HIV PrEP for claims may include:
| Code | Narrative |
|---|---|
| J0739 | Injection, cabotegravir, 1mg, FDA approved prescription, only for use as HIV pre-exposure prophylaxis (not for use as treatment for HIV) |
| G0011 | Individual counseling for pre-exposure prophylaxis (PrEP) by physician or QHP [qualified health professional] to prevent human immunodeficiency virus (HIV), includes: HIV risk assessment (initial or continued assessment of risk), HIV risk reduction and medication adherence, 15-30 minutes |
| G0013 | Individual counseling for pre-exposure prophylaxis (PrEP) by clinical staff to prevent human immunodeficiency virus (HIV), includes: HIV risk assessment (initial or continued assessment of risk), HIV risk reduction and medication adherence |
| G0012 | Injection of pre-exposure prophylaxis (PrEP) drug for HIV prevention, under skin |
Diagnosis codes are required for claims submitted to Medicare. A new diagnosis code recently became available (Z29.81: Encounter for HIV pre-exposure prophylaxis).
Resources
- Providers can learn more at cms.gov/medicare/coverage/prep.
- Members can learn more by going to our Medicare Options website.
MPC_090924-3U-1
This article is for acute care hospitals, ambulatory surgical centers, and out-of-network providers caring for our members
The No Surprises Act, enacted as part of the Consolidated Appropriations Act (CAA) in late 2020, provides new federal consumer protections against balance billing for medical bills under certain circumstances. Claims subject to balance billing protections may occur:
- In emergency situations when a patient can’t control who is involved in their care
- In non-emergency situations when they schedule a visit at an in-network facility but are unexpectedly treated by an out-of-network provider
- When out-of-network air ambulance services are provided for services that would have been covered if the air ambulance provider was in-network
Ground ambulance claims are not included under the No Surprises Act.
We want to let you know how we’re educating our members about their rights and protections under the law. We are posting disclosures explaining the rights and protections our members have under the law to our public website in late December: https://www.bluecrossma.org/disclaimer/member-rights. Our Explanation of Benefits (EOB) when we pay bills covered by the law will direct members to the following explanation of the law:
Emergency services
If you have an emergency medical condition and get emergency services from an
out-of-network provider or facility, the most the provider or facility may bill
you is your plan’s in-network cost-sharing amount (such as copayments and
coinsurance). You can’t be balance billed for these emergency services.
This includes services you may get after you’re in stable condition, unless you
give written consent and give up your protections not to be balanced billed for
these post-stabilization services.
Certain services at an in-network hospital or ambulatory surgical center
When you get services from an in-network hospital or ambulatory surgical center,
certain providers there may be out-of-network. In these cases, the most those
providers may bill you is your plan’s in-network cost-sharing amount. This
applies to emergency medicine, anesthesia, pathology, radiology, laboratory,
neonatology, assistant surgeon, hospitalist, or intensivist services. These
providers can’t balance bill you and may not ask you to give up
your protections not to be balance billed. If you get other services at these
in-network facilities, out-of-network providers can’t balance bill you, unless
you give written consent and give up your protections.
You’re never required to give up your protections from balance billing. You also aren’t required to get care out-of-network. You can choose a provider or facility in your plan’s network.
When balance billing isn’t allowed, you also have the following protections:
- You are only responsible for paying your share of the cost (like the copayments, coinsurance, and deductibles that you would pay if the provider or facility was in-network). Your health plan will pay out-of-network providers and facilities directly.
- Your health plan generally must:
- Cover emergency services without requiring you to get approval for services in advance (prior authorization).
- Cover emergency services by out-of-network providers.
- Base what you owe the provider or facility (cost-sharing) on what you would pay an in-network provider or facility and show that amount in your explanation of benefits.
- Count any amount you pay for emergency services or out-of-network services toward your deductible and out-of-pocket limit.
Non-participating providers’ responsibilities and rights under the law
Under the No Surprises Act, non-participating providers are prohibited from balance billing under the circumstances described above.
The statute requires providers, including hospitals, to make notice about balance billing requirements and prohibitions publicly available and provide them to consumers. The regulations supporting the No Surprises Act detail information that must be included in such notice.
The federal law also includes provisions allowing providers to request negotiation of the payor’s payment for bills subject to the No Surprises Act, and if negotiation fails, to enter into the Independent Dispute Resolution (IDR) process, also known as arbitration, to determine the allowed payment amount.
- If the provider or facility wishes to initiate a 30-day open negotiation period for purposes of determining the amount of total payment, please contact:
Mail: Blue Cross Blue Shield of MA
Provider Appeals
PO Box 986065
Boston, MA 02298Phone: 1-800-882-2060 (physicians)
1-800-451-8123 (hospitals)
1-800-451-8124 (ancillary providers)Email: PSRequest@bcbsma.com The request should include both the Open Negotiation Notice and the Request for Claim Review forms.
- If that 30 day open negotiation period does not result in a determination, generally the provider or facility may initiate the IDR process within 4 days after the end of the open negotiation period. To initiate the IDR process, submit requests in writing to:
- Email - NSAIDR@multiplan.com
Resources
- cms.gov/nosurprises
- We've added this information to the Billing Guidelines and Resources section of our website
MPC_102021-2R-1
This article is for acute care facilities, ambulance service suppliers, dialysis facilities, extended care facilities, home health agencies, long term care hospitals, rehabilitation hospitals, and urgent care centers caring for our members
For the duration of the Massachusetts health emergency, we will waive pre-authorization requirements for ground ambulance transport by a contracted provider. In addition, ground ambulance transport to and from the locations listed below will be covered to help our healthcare delivery system optimize inpatient capacity.
- Applies to in-network, ground ambulance providers for HMO, PPO, Indemnity, Medicare Advantage, and Federal Employee Program* members
- Excludes air ambulance transport
- Notification is not required
- Cost share is waived for members with a COVID-19 diagnosis
- Cost share will apply to members without a COVID-19 diagnosis.
How to bill for ambulance transport
Be sure to bill using CPT A0426, A0428, A0433, or A0434 (non-emergent transports) and the appropriate modifier shown below to represent the direction of the transfer.
August 18, 2020 update: The modifiers NJ and JN were added to the table below. Refer to our August 18, 2020 news article for this update.
| Modifier | Description |
|---|---|
| DH | Diagnostic site (including COVID-19 testing) or therapeutic site (including dialysis; excluding physician office or hospital) to hospital |
| EH | Residential, domiciliary, custodial facility (other than skilled nursing facility) if the facility is the beneficiary’s home to hospital |
| HD | Hospital to diagnostic site (including COVID-19 testing) or therapeutic site (including dialysis; excluding physician office or hospital) |
| HE | Hospital to residential, domiciliary, custodial facility (other than skilled nursing facility) if the facility is the beneficiary’s home |
| HH | Hospital to hospital (includes ASCs approved to provide hospital level of care) |
| HN | Hospital to alternative site for skilled nursing facility (SNF) |
| HR | Hospital to residence |
| JN* | Freestanding end-stage renal disease (ESRD) facility to skilled nursing facility |
| NH | Alternative site for SNF to hospital |
| NJ* | Skilled nursing facility to freestanding end-stage renal disease (ESRD) facility |
| NN | SNF to SNF |
| NR* | SNF to residence |
| PD | Physician office to community mental health center, federally qualified health center, rural health center, urgent care facility, non-provider-based ambulatory surgical center or freestanding emergency center, or location furnishing dialysis services that is not affiliated with an end-stage renal facility |
| PE* | Physician office to residential, domiciliary, custodial facility (other than skilled nursing) if the facility is the beneficiary’s home |
| PH | Physician office to hospital |
| PR* | Physician office to home |
| RH | Residence to hospital |
| RN* | Residence to SNF |
*These modifiers do not apply to Federal Employee Program members.
MPC_030620-1N-28
This article is for dentists and oral surgeons caring for our members
Periodically, we’ll bring you important information to help you improve the way we work together . The table below explains some common reasons why claims are rejected. It shows the Provider Detail Advisory/Provider Voucher messages you’ll receive for each and best practices for how to resolve the problem.
| When the rejection code and message is | This means that | And you should |
|---|---|---|
| U301: According to our records, we have already processed a claim for this service. Please check your records for a previous claim submission. | We have more than one claim on file for this patient for this service. |
|
| M020: The benefit dollar maximum has been reached. | The member has spent all the available dollars for their policy | You can bill the member up to the plan allowable fee for services until their new plan year |
| E240: Policy not active for the date of service. Please verify prefix and identification number and resubmit your claim. | The member did not have insurance with us at time of service | Confirm that you submitted the correct information on the claim. If the information was:
|
Resources
Log in for access to secure resources.
![]() Dental Blue Book()
Dental Blue Book()
![]() CDT Coding Guidelines()
CDT Coding Guidelines()![]() Sample Provider Detail Advisory
Sample Provider Detail Advisory
To verify claims payment and search for claims, refer to payspan.com.
To verify benefits, eligibility, and claim status, use an eTool like Dental Connect().
MPC_031120-1L-7
Periodically we bring you important information to help you avoid having your claims rejected. Below is the second article of three parts that explain some common reasons why claims are rejected and the Provider Detail Advisory/Provider Voucher messages you’ll receive for each. (See the first part here.) We’ve also outlined best practices for how to resolve the problem.
| When the rejection code and message is | This means that | And you should |
|---|---|---|
| X419: Your NPI and tax ID combination do not match the information we have on file. Please verify the NPI and tax ID and submit a new claim. | We do not have the same NPI and tax identification on file as what you submitted | List the practice NPI in box 49. For sole proprietors, report the individual NPI in box 49. Validate all software programs for the correct information prior to claim resubmitting the claims. Refer to Section 5 of the Blue book for proper billing guidelines. |
| F042: We can't identify the member from the ID number submitted. Please verify eligibility by using online services at Bluecrossma.com/provider (log in required). Please submit a new claim with the correct id number. | We cannot find a member that has insurance with us at time of service | Confirm that the correct information was submitted on the claim. If the information was:
|
| B415: The patient’s plan does not cover this dental procedure. Or E232: This is not a covered benefit. |
The member does not have benefits for this procedure on their policy with us | You may bill the member for service. |
Resources:
Dental Blue Book
CDT Coding Guidelines
To verify claims payment and search for claims, refer to payspan.com
To verify benefits, eligibility, and claim status on Dental Connect
MPC_031120-1L-8
This article is for dentists and oral surgeons caring for our members
Periodically we’ll be bringing you important information to help you avoid having your claims rejected. Below we’ve explained some common reasons why claims are rejected, and the Provider Detail Advisory/Provider Voucher messages you’ll receive for each. We’ve also outlined best practices for how to resolve the problem.
| When the rejection code and message is | This means that | And you should |
|---|---|---|
| B592: This service is not a covered benefit when performed on a patient of this age. | The patient is not old enough for the service that is being billed | Confirm that the procedure code and tooth number combination being billed is correct.
|
| X284: We are unable to pay for this service without additional information the procedure you have submitted requires a valid tooth number(s), quadrant or arch identification and/or tooth surface(s). Please resubmit a claim for this service with the required information for processing. Thank you. | The procedure code needs additional information so we can process the claim correctly. | Confirm that the procedure code and tooth number/ surface or additional identifiers are being billed is correctly. If the information is:
|
Resources:
![]() Dental Blue Book
Dental Blue Book
![]() CDT Coding Guidelines
CDT Coding Guidelines
To verify claims payment and search for claims, refer to www.payspan.com
To verify benefits, eligibility, and claim status on Dental Connect
![]() Dental Blue Book
Dental Blue Book ![]() CDT Coding Guidelines
CDT Coding Guidelines
To verify claims payment and search for claims, refer to payspan.com
To verify benefits, eligibility, and claim status on Dental Connect
MPC_031120-1L-9-ART
This article is for physicians, clinicians, and durable medical equipment providers ordering and supplying BPAP, CPAP, and mechanical ventilators for our members
 Philips Respironics issued a voluntary recall (philips.com/src-update) of devices used to treat obstructive sleep apnea due to issues related to sound abatement foam used in some devices. The recall includes certain:
Philips Respironics issued a voluntary recall (philips.com/src-update) of devices used to treat obstructive sleep apnea due to issues related to sound abatement foam used in some devices. The recall includes certain:
- Bi-level positive airway pressure (BPAP) devices
- Continuous positive airway pressure (CPAP) devices
- Mechanical ventilators
Because this is a manufacturer’s recall, Philips will be responsible for any replacement devices.
Costs associated with this recall are not the responsibility of the member or Blue Cross Blue Shield of Massachusetts.
Supporting our members using these devices
Members will need to work with their durable medical equipment provider (who will work with Philips) to receive a replacement device, when applicable.
An impacted member should speak to the doctor who ordered their device about any risks or benefits of continuing to use it or their options while waiting for a new device.
What should durable medical equipment (DME) providers do?
DME providers should identify all recalled devices provided to members and immediately take the following actions:
- Mail the Philips recall notification letter to the patient (our member).
- Register all recalled devices with Philips Respironics.
- Increase community recall awareness via phone messaging, staff messaging, email, text, websites, and social media where possible.
- Help members with recall information and registering their devices, whenever possible.
Additional information
| For | Then |
|---|---|
| PAP devices less than five years old |
|
| Devices more than five years old |
|
| Rental devices (not considered purchased) |
|
| PAP supplies for devices associated with the recall |
|
Resources
- Philips Respironics recall website
- Philips Respironics home page
- Centers for Medicare & Medicaid
Services Frequently Asked Questions about the recall
- U.S. Food and Drug Administration safety communication
Questions
Contact durable medical equipment network representative, Odette Palmer-Lee, at Odette.Palmer-Lee@bcbsma.com or call 1-617-246-5711.
MPC_070921-2W-1
This article is for durable medical equipment suppliers
Blue Cross covers pneumatic compression pumps for treatment of lymphedema and venous ulcers (Medical policy 354) and postsurgical home use of limb compression devices for venous thromboembolism prophylaxis (Medical policy 541).
As a reminder, the medical policies describe conditions that must be met for these devices to be covered for our commercial members:
- Medical policy 354: Pneumatic compression pumps are covered for the treatment of lymphedema.
- Medical policy 541: Limb compression devices are covered in the home setting for the prevention of venous thromboembolism (VTE) after a major orthopedic or non-orthopedic surgery for patients who are at moderate or high risk of VTE.
Payment policy application
- Enforcement of this medical policy occurs through system edits and post-payment reviews.
- We continually expand our ability to process claims in accordance with this policy pre-payment, which will reduce the number of claims we review post-payment.
Resources
The included HCPCS codes and diagnoses are listed on their respective medical policies, which will be updated on our website on October 15. To download these medical policies, log in and click Find a Medical Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Medical Policies.
MPC_090821-1V-1-ART
This article is for all providers, except behavioral health providers and dentists.
As required by the National Committee for Quality Assurance (NCQA), we will start to collect medical record information for the Healthcare Effectiveness Data and Information Set (HEDIS) audit in February 2024. Submitting your medical records promptly to us is important. Please respond to record requests within three weeks to ensure all necessary documents are submitted.
HEDIS is one of the ways we measure the quality of care you provide to our members and is a very important activity for all NCQA-accredited health plans.
As a reminder, complying with medical record requests from Blue Cross to support medical management, quality management, compliance, and other programs is a part of your provider Agreement with us. If you use a vendor for your medical records, be sure they know that they cannot bill us for the records.
We recommend remote submission
We partner with several provider organizations and hospitals to receive direct electronic medical records (EMR) access, which allows us to extract only the required information we need. This method eliminates the need for your office staff to pull medical records and send them to us, saving resources for your individual practices.
For more information on setting up remote EMR access, please contact Karen Sulham at 1-617-246-4409.
Not able to submit remotely?
If remote submission is not an option for your organization, secure email, or fax is available. We can also set up a secure file transmission process (eSFTP) for larger volumes of records. For smaller volumes, please use our secure email or fax line, as the most efficient way to return records to us.
If you work with a third-party vendor to share medical records, please instruct them to return the charts by
- Setting up eSFTP,
- Sending a secure email to HEDIS@bcbsma.com, or
- Faxing records to 1-888-641-4990.
Reminder about privacy laws
The Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule has national standards to protect patients’ personal health information. Per HIPPA requirements, please send only the minimum amount of protected health information needed to meet this request.
Questions?
If you have any questions or would like to discuss which medical record collection option is best for your practice, please call our Blue Cross HEDIS Team at 1-888-994-3347.
Thank you in advance for responding promptly to this request.
MPC_103023-1B-1
This article is for all professional and outpatient facility providers
Prolonged service and visit complexity codes
For 2021, the American Medical Association and the Centers for Medicare & Medicaid Services have released new CPT and HCPCS codes for prolonged evaluation and management (E/M) and visit complexity inherent to E/M.
Beginning January 1, 2021, we will reimburse for visit complexity inherent to the E/M service (HCPCS G2211) for Medicare Advantage products only.
| Code | Narrative |
|---|---|
| G2211 | Visit complexity inherent to evaluation and management associated with medical care services that serve as the continuing focal point for all needed health care services and/or with medical care services that are part of ongoing care related to a patient’s single, serious, or complex chronic condition) |
Consistent with our existing payment policy, we will not reimburse the new prolonged E/M service codes 99417 and G2212 that are effective January 1, 2021.
| Code | Narrative |
|---|---|
| 99417 | Prolonged office or other outpatient evaluation and management service beyond the minimum required time of the primary procedure which has been selected using total time |
| G2212 | Prolonged office or other outpatient evaluation and management service(s) beyond the maximum required time of the primary procedure which has been selected using total time on the date of the primary service; each additional 15 minutes by the physician or qualified healthcare professional, with or without direct patient contact |
E/M guideline reminder
We notified you on September 1 that Blue Cross would adopt the 2021 American Medical Association new guidelines for outpatient evaluation and management code selection. As a reminder, professional RVU and fee updates will follow our normal update schedule:
- Commercial professional fee update will be September 1, 2021
- Medicare Advantage professional fee update will be January 1, 2021
To access this News Alert, log in and go to News. Look for the September 1 News Alert called "2021 evaluation and management guidelines update."
Resources
- For detailed information about these changes, please refer to the AMA website.
- We will update our Evaluation and Management Services payment policy with this information. To download this payment policy, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_092520-5C-1
This article is for primary care providers, mental health care clinicians and physicians, acute care hospitals, and mental health facilities caring for our members
Effective immediately, we’re waiving member cost share for services billed with the following codes:
| Collaborative Care Management | Care Management | Interprofessional telehealth assessment and management services when billed by mental health providers and facilities |
|---|---|---|
|
|
|
We believe that this change will:
- improve our members’ access to mental health care by removing cost barriers for members seeking mental health treatment
- prevent members from receiving bills for services for which they don’t expect to pay a cost share
- encourage and support the integration of mental health care into primary care.
| Code | Description |
|---|---|
| 99446 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 5-10 minutes of medical consultative discussion and review |
| 99447 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 11-20 minutes of medical consultative discussion and review |
| 99448 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 21-30 minutes of medical consultative discussion and review |
| 99449 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a verbal and written report to the patient's treating/requesting physician or other qualified health care professional; 31 minutes or more of medical consultative discussion and review |
| 99451 | Interprofessional telephone/internet/electronic health record assessment and management service provided by a consultative physician, including a written report to the patient's treating/requesting physician or other qualified health care professional, 5 minutes or more of medical consultative time |
| 99452 | Interprofessional telephone/internet/electronic health record referral service(s) provided by a treating/requesting physician or other qualified health care professional, 30 minutes |
| 99484 | Care management services for behavioral health conditions, at least 20 minutes of clinical staff time, directed by a physician or other qualified health care professional, per calendar month, with the following required elements: initial assessment or follow-up monitoring, including the use of applicable validated rating scales, behavioral health care planning in relation to behavioral/psychiatric health problems, including revision for patients who are not progressing or whose status changes, facilitating and coordinating treatment such as psychotherapy, pharmacotherapy, counseling and/or psychiatric consultation, and continuity of care with a designated member of the care team. |
| 99492 | Initial psychiatric collaborative care management, first 70 minutes in the first calendar month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional, with the following required elements: outreach to and engagement in treatment of a patient directed by the treating physician or other qualified health care professional, initial assessment of the patient, including administration of validated rating scales, with the development of an individualized treatment plan, review by the psychiatric consultant with modifications of the plan if recommended, entering patient in a registry and tracking patient follow-up and progress using the registry, with appropriate documentation, and participation in weekly caseload consultation with the psychiatric consultant, and provision of brief interventions using evidence-based techniques such as behavioral activation, motivational interviewing, and other focused treatment strategies. |
| 99493 | Subsequent psychiatric collaborative care management, first 60 minutes in a subsequent month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional, with the following required elements: tracking patient follow-up and progress using the registry, with appropriate documentation, participation in weekly caseload consultation with the psychiatric consultant, ongoing collaboration with and coordination of the patient's mental health care with the treating physician or other qualified health care professional and any other treating mental health providers, additional review of progress and recommendations for changes in treatment, as indicated, including medications, based on recommendations provided by the psychiatric consultant, provision of brief interventions using evidence-based techniques such as behavioral activation, motivational interviewing, and other focused treatment strategies, monitoring of patient outcomes using validated rating scales, and relapse prevention planning with patients as they achieve remission of symptoms and/or other treatment goals and are prepared for discharge from active treatment. |
| 99494 | Initial or subsequent psychiatric collaborative care management, each additional 30 minutes in a calendar month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional (List separately in addition to code for primary procedure) |
| G0512 | Rural health clinic or federally qualified health center (RHC/FQHC) only, psychiatric collaborative care model (psychiatric COCM), 60 minutes or more of clinical staff time for psychiatric COCM services directed by an RHC or FQHC practitioner (physician, NP, PA, or CNM) and including services furnished by a behavioral health care manager and consultation with a psychiatric consultant, per calendar month |
| G2214 | Initial or subsequent psychiatric collaborative care management, first 30 minutes in a month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional |
Resources
For more information about our coverage of interprofessional telehealth assessment and management services, please see our November 2, 2022 news article.
You may also wish to refer to our related payment policies:
- Mental Health and Substance Use payment policy
- Non-Reimbursable Services payment policy
- Telehealth (Telemedicine) - Mental health payment policy
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
MPC_071720-1B-2
This article is for technical diagnostic imaging facilities and multi-specialty physician groups caring for our members
Based on our review of claims processed for A9587 (Gallium GA-68, dotatate, diagnostic, 0.1 millicurie), we will update our reimbursement for A9587 on October 1, 2021. On that date, we will move from a global payment to a per unit cost. This change applies to all products.
| Code | Current Fee | New rate, effective October 1, 2021 |
|---|---|---|
| A9587 | $3,604.00 | $66.74 per unit |
Our review of prior claims found that some providers who had billed for more than one unit of A9587 were reimbursed more than the global fee of $3,604. We will retrospectively adjust claims billed with multiple units prior to October 1, 2021 to allow only one unit of service at the current fee ($3,604). If you have affected claims, your claim will be adjusted so that you receive the global payment of $3,604.
MPC_072721-1R-1
We have updated our General Coding and Billing Payment Policy with information about National Physician Fee Schedule File professional component (PC) and technical component (TC) indicator 3 codes.
We want to remind you that Blue Cross does not reimburse any CPT or HCPCS codes identified as having a professional or technical indicator of 3 (PC/TC 3) in a facility setting. We have aligned our operations to support this policy.
PC/TC 3 codes represent the technical component of a service. That service has a different CPT or HCPCS code representing the professional component of the service. These technical codes have no associated physician work relative value units (RVUs) and therefore will not be reimbursed.
This policy applies to all products.
What codes apply?
|
G0128 G0248 G0249 G0277 G0288 G0404 G0472 G2066 G6003 G6004 G6005 G6006 G6007 G6008 G6009 G6010 G6011 G6012 G6013 G6014 G6015 |
G6016 Q0092 R0070 R0075 0208T 0209T 0210T 0211T 0212T 0497T 0502T 0503T 0541T 0624T 0625T 20697 36591 36592 36593 51798 77336 |
77370 77371 77372 77373 77385 77386 77401 77402 77407 77412 77417 77423 77520 77522 77523 77525 77790 86485 86486 86490 86510 |
86580 88184 88185 89220 89230 92227 92229 92547 92552 92553 92555 92556 92561 92562 92563 92564 92565 92571 92572 92575 92576 |
92577 92582 92583 92596 93005 93017 93041 93225 93226 93229 93242 93243 93246 93247 93270 93271 93296 93668 93701 93702 93786 |
93788 93792 94015 94760 94761 94762 94775 94776 95028 95060 95065 95070 95249 95250 96127 96932 96935 99153 99415 99416 |
Resources
To access our payment policies, login and go to Office Resources>Policies & Guidelines>Payment Policies
- General coding and billing payment policy
- Non-reimbursable services payment policy
Questions?
If you have any questions, please call Provider Services at the appropriate number:
- Physicians: 1-800-882-2060
- Hospitals: 1-800-451-8123
- Ancillary providers: 1-800-451-8124
As always, thank you for the care you provide to our members.
MPC_040621-1N-1
This article is for anesthesiologists and gastroenterologists caring for our members
As a reminder, effective January 1, 2024, we will implement diagnosis-driven claim edits to reinforce our existing monitored anesthesia care (MAC) medical policy 154 guidelines.
For our enforcement of this policy on January 1, 2024, it’s important to know that we cover monitored anesthesia care for endoscopic procedures such as colonoscopies and upper endoscopies when medically necessary. Medical policy 154 lists diagnosis codes and clinical scenarios where monitored anesthesia care is medically necessary for endoscopic procedures, outlined by certain medical conditions and complication risks.
Our medical policy aligns with the American Society of Gastrointestinal Endoscopy (ASGE), American College of Gastroenterology, American Gastroenterological Association, and American Society of Anesthesiologists (ASA) guidelines.
Why are we implementing this enforcement?
- In accordance with the above guidelines, endoscopic procedures can be performed under either moderate sedation or monitored anesthesia care.
- In appropriately selected patients, moderate sedation is comparably safe and more cost effective than monitored anesthesia care.
- The member’s cost share is the same for either monitored anesthesia care or moderate sedation, and the amount is based on their plan benefits.
- Note: If an endoscopic procedure is performed under monitored anesthesia care and does not align with medical policy 154, the member is not liable for the non-covered amount.
As a result of processing claims in accordance with our policy on a pre-payment basis, we are able to reduce the number of claims needing post-payment review.
Resources
- Medical policy 154 - Monitored Anesthesia Care (MAC)
- May 19 article: We are postponing our monitored anesthesia care claim edits
MPC_120522-1Q-5-ART
This article is for all providers caring for our members
As you know, Blue Cross reimburses NOC (not otherwise classified) or unlisted CPT and HCPCS codes only when submitted with supporting documentation. We previously informed you about our revised, clarified guidelines. As a reminder, you need to follow these guidelines when submitting documentation for NOC codes to allow for a more efficient, timely, and accurate review.
For electronic claims, you may submit an appeal with supporting documentation. For paper claims, you may either submit the documentation with the claim itself, or in a separate appeal.
NOC code supporting documentation guidelines
Because unlisted codes do not describe a specific procedure or service, supporting documentation must contain clear, identifying information. You should provide a detailed description of what the NOC code represents, along with circled or underlined notes that identify the test or procedure associated with the unlisted code. The notes must be legible and contain the minimum necessary information to support the NOC code.
| For example, if you are billing | Then submit a description, such as | Along with |
|---|---|---|
| Unlisted CPT code 31599 | Unlisted procedure, endoscopic supraglottoplasty | Circled or underlined notes that identify the service |
Make sure that your NOC code supporting documentation includes or meets the below criteria.
- A detailed description of the type and extent of the procedure or service.
- When available, a similar or ‘treat-like’ code for the service represented by the NOC code.
- Documentation should be specific to the procedure or service performed. Non-pertinent information should be omitted.
- Identify when the procedure was performed independently from other services provided, or if it was performed at the same surgical site or opening.
- Time, effort, and equipment necessary to provide the service, including any extenuating circumstances which may have complicated the service or procedure.
- The number of times the service was provided.
- For drug NOC codes, NDC number is required.
If your supporting documentation does not adhere to these requirements, your claim’s processing will be impacted, with high potential for claim denial.
Resources
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE(2583). As always, thank you for the care you provide to our members.
MPC_120524-1D-1
This article is for acute care facilities caring for our members
Blue Cross reimburses for evaluation and management (E/M) services as outlined in our existing Outpatient Clinic Services – Facility Payment Policy.
As a reminder, we only reimburse E/M services in a facility setting when billed with professional revenue codes.
Our existing Outpatient Clinic Services – Facility Payment Policy states the following:
- Blue Cross reimburses E/M services billed with a professional revenue code only.
- Blue Cross does not reimburse facility charges for E/M services performed in any outpatient setting.
Payment policy application
In Q2 2022, we will have the ability to process claims in accordance with this payment policy pre-payment. We will also enforce our existing policy through post-payment reviews.
See our payment policy for additional reimbursement and billing guidelines.
Questions?
Call Provider Service at 1-800-882-2060. As always, thank you for the care you provide to your patients—our members.
Resources
Outpatient Clinic Services – Facility Payment Policy (log in and go to Office Resources>Policies & Guidelines>Payment Policies).
MPC_111821-2A-1
This article is for acute care facilities caring for our members
Blue Cross reimburses for outpatient rehabilitation services as outlined in our existing Outpatient Rehabilitation Services payment policy.
As a reminder, we reimburse:
- Initial evaluation for physical or occupational therapy
- Physical therapy treatment with one rate that includes all modalities rendered, per member, per date of service
- Both the initial evaluation and therapy treatments rendered on the same day for the same member by the same provider
- Occupational therapy treatment with one rate that includes all modalities rendered, per member, per date of service
- Speech therapy treatment
We do not reimburse:
- Dry hydrotherapy
Billing information
| Revenue codes | Description | Comments |
|---|---|---|
| 0421 | Physical therapy – visit charge | Bill one unit of service, regardless of the number of modalities rendered, with the sum of all applicable charges. Reimbursable with the initial evaluation if it occurs on the same day as the treatment. |
| 0424 | Physical therapy – evaluation or reevaluation | |
| 0431 | Occupational therapy – visit charge | Bill one unit of service, regardless of the number of modalities rendered, with the sum of all applicable charges. Reimbursable with the initial evaluation if it occurs on the same day as the treatment. |
| 0434 | Occupational therapy – evaluation or reevaluation |
See our payment policy for additional reimbursement and billing guidelines.
Questions?
Call Provider Service at 1-800-882-2060. As always, thank you for the care you provide to your patients—our members.
Resources
MPC_050422-2I-1
This article is for all providers caring for our members
Blue Cross accepts industry-standard modifiers to allow for clear provider reporting of services and accurate claims processing. When a CPT or HCPCS modifier is reported on a professional or facility claim, the applicable reimbursement information applies to all provider types.
As a reminder, our CPT and HCPCS Modifiers payment policy states:
- Modifiers may affect how claims are processed, how services are priced, and how payment is calculated. Modifiers can also affect how we apply member benefits.
- Claims submitted with modifiers are subject to pre and/or post-pay audit. Medical notes must support services identified by the modifier.
- Blue Cross accepts all standard current procedural terminology (CPT) and healthcare common procedure coding system (HCPCS) modifiers submitted in accordance with the appropriate procedure codes. Certain modifiers, when submitted appropriately, will impact reimbursement.
- The absence or presence of a modifier may result in a claim denial.
Refer to our existing CPT and HCPCS Modifiers payment policy for additional guidelines.
Payment policy application
We have expanded our ability to process claims pre-payment in accordance with our existing payment policy. As a result, this will help reduce the number of claims that need post-payment review.
Resources
- CPT and HCPCS Modifiers payment policy
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_031124-1V-1-ART
This article is for acute care hospitals caring for our members
Blue Cross reimburses for emergency room services as outlined within our existing Emergency Room - Facility payment policy.
As a reminder, our payment policy states that Blue Cross:
- Reimburses emergency room services, which include:
- Room and facility charges that are directly related to the emergency, or
- Procedures performed in the emergency room, such as surgeries, treatments, and therapies.
- Separately reimburses ancillary services performed during an emergency room visit, such as laboratory and radiology work.
- Does not separately reimburse for services, products, or drugs considered incidental to the emergency procedure performed.
Payment policy application
Starting in Q1 2024, we will process claims pre-payment in accordance with our existing policy and will no longer separately reimburse services, products, or drugs considered incidental to the emergency room procedure performed. As a result, this will help reduce the number of claims that need post-payment review.
Resources
- Emergency Room - Facility payment policy
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_101823-1F
This article is for providers who perform obstetric services for our members
When billing for obstetric evaluation and management (E/M) services, please review our existing Obstetrical and Maternity Care payment policy. E/M codes are not routinely reimbursed separately from the global obstetric service.
As a reminder, global obstetric services are reimbursed at an all-inclusive rate and include:
- Monthly visits up to 28 weeks of gestation
- Biweekly visits up to 36 weeks of gestation
- Weekly visits until delivery and up to 42 days post-delivery
Only E/M visits that are related to a current complication are reportable. Do not report visits in which the monitoring of a potential problem does not result in a complication.
Refer to our Obstetrical and Maternity Care payment policy for additional billing guidelines. To download this policy, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines> Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_082223-2S-1
This article is for acute care hospitals where our members receive observation care
Blue Cross Blue Shield of Massachusetts reimburses for observation services as outlined in our observation payment policy.
As a reminder, our existing observation payment policy states that Blue Cross does not reimburse observation services when rendered as part of normal recovery.
- Enforcement of this policy has previously been done through post payment audits.
- Blue Cross now has the ability to configure our system to process claims in accordance with the payment policy referenced above.
- You will begin to notice pre-payment enforcement soon. This will reduce the number of observation post payment audits.
Remember these important billing requirements
- When billing for observation services, please make sure you are evaluating for medical necessity criteria.
- Report the observation stay using hours, rounded to the nearest hour.
- Report observation services using only revenue code 0762 and the appropriate observation CPT or HCPCS code noted within the policy.
- Report all outpatient facility services related to the observation stay on the same claim form.
Questions?
Call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to your patients—our members.
Resources
Observation payment policy (log in required)
MPC_092520-3N-1-ART
Please share this communication with your billing department or billing agency.
We’ve been requiring you to submit replacements to correct previously submitted CMS-1500 and UB-04 claims for several years. We'd like to remind you about specific scenarios where you cannot follow this process.
Reminder of when not to use replacements
You cannot use replacement claims to:
- Change or correct the:
- Billing NPI
- Date of service (when it falls outside the original date span)
- Level of care (inpatient to outpatient, or vice versa)
- Subscriber ID
- Submit an appeal or review (examples: timely filing, individual consideration)
- Change a bridged admission claim
- Correct a claim that was part of a previous recovery or audit
- Correct BlueCard claims that denied for referral or authorization
Please use replacement claims for all other corrections.
Resources
- Replacement claim requirement frequently asked questions (recently revised)
- Checking claim status (new)
- Payspan quick start guide (recently revised)
- How to correct rejected claims
MPC_012420-1P-7
This article is for dermatologists and podiatrists caring for our members
On January 1, 2024, we will update our medical policy 707 to include specific criteria that determine medical necessity for the removal of benign skin lesions. This change applies to commercial (HMO, PPO, Indemnity) products only.
The covered criteria that will be added to the policy includes:
- Clinical suspicion of a malignancy
- Known pre-malignant lesions
- Functional limitation and risk for infection transmission
- Symptoms as evidenced by bleeding, redness, pain, etc.
Enforcement of this policy will begin January 1, 2024 through the use of diagnosis-driven claim edits. Our updated Medical policy 707 – Benign Skin Lesions will be available for reference on January 1, 2024.
MPC_080123-1T-1
To align with the Division of Insurance, Blue Cross has revised our rates for COVID-19 vaccine administration codes effective April 1, 2021.
Professional Temporary COVID-19 fee schedule updates
![]() Temporary COVID-19 Professional Commercial and FEP Fee Schedule During COVID-19 Public Health Emergency
Temporary COVID-19 Professional Commercial and FEP Fee Schedule During COVID-19 Public Health Emergency
To access the fee schedule updates, log in and go to Office Resources>Billing & Reimbursement>Fee Schedules.
Hospital Temporary COVID-19 fee schedule updates
- Please contact your network representative for the updated hospital outpatient fee schedule.
MPC_030620-1N-181
This article is for providers caring for our Medicare Advantage members
Risk adjustment is a payment methodology used by the Centers for Medicare & Medicaid Services to ensure health plans are reimbursed appropriately for Medicare Advantage members.
We recently added a risk adjustment resource page to Provider Central. Log in and navigate to Quality & Performance>Quality Indicators>Risk Adjustment Documentation & Coding. The page covers:
- What is risk adjustment?
- Why is it important?
- Remote submission
- Telehealth
- Coding tip flashcards on:
- Chronic kidney disease
- Deep vein thrombosis
- Diabetes
- Fracture
- Major depressive disorder
- Status codes
- TAMPERTM
- Unconfirmed diagnosis
- Using active voice
We’ve also given you links to two fact sheets: Risk Adjustment and In-home care program with Signify HealthTM.
Questions on documentation and coding?
Send an email to the Risk Adjustment Coding Quality Education Team.
As always, thank you for the care you provide to our members.
MPC_100620-1P-15
This article is for podiatrists caring for our Medicare Advantage members

Recently, we’ve noticed an increased number of podiatrists submitting claims for non-covered routine foot care for Medicare Advantage members. Since Medicare generally excludes coverage for routine foot care, this results in denied claims with members receiving unexpected charges.
As a reminder, routine foot care includes:
- Cutting or removing corns and calluses
- Trimming, cutting, or clipping nails
- Hygienic or preventive maintenance, like cleaning or soaking feet
Medical Necessary coverage
Payment may be made for routine foot care when the patient has a systemic disease—such as metabolic, neurologic, or peripheral vascular disease—of sufficient severity that performance of such services by a nonprofessional person would put the patient at risk (for example, a systemic condition that has resulted in severe circulatory embarrassment or areas of desensitization in the patient’s legs or feet).
For Medicare Advantage members, providers should follow the appropriate local coverage determination (LCD) prior to rendering services to determine if the services meet medically necessity guidelines.
Related medical policy
![]() Medical
policy 132, Medicare Advantage Management
Medical
policy 132, Medicare Advantage Management
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_072224-1Y-1-ART
This article is for dentists and oral surgeons caring for our members
We know that a pain point for dental offices and their billing agencies is spending time calling us to find out our procedure guidelines and submission requirements. We’re proud to launch a simple, online CDT look-up tool to make this task less time-consuming!
While our phone representatives currently provide procedure guidelines for up to 10 codes each time you call, you can use the online tool for as many codes as needed, saving you time. You can access the tool 24/7 from Provider Central by going to: Office Resources > Billing & Reimbursement > CDT Dental Procedure Code Lookup.
Using the tool is as simple as 1-2-3!
|
Step |
Use Dental Connect to find the name of the member’s plan. This may be different than what’s shown on the member’s ID card. This will ensure that you get the most accurate information. |
|
Step |
Use the pull-down menu to enter the plan name from Step 1. The plan name determines whether the member’s plan uses our standard CDT guide or our Pediatric Essential CDT Guide. For a small number of plans, you’ll need to call Dental Provider Services to find out which guide to use. |
|
Step |
Enter the CDT code starting with the letter “D.” As you type more digits, you’ll narrow your results. If you want to see all the codes in a range of services, just type “D” plus the first 2 or three digits of the code. |
For members covered under our standard dental plans, your results will look like this:
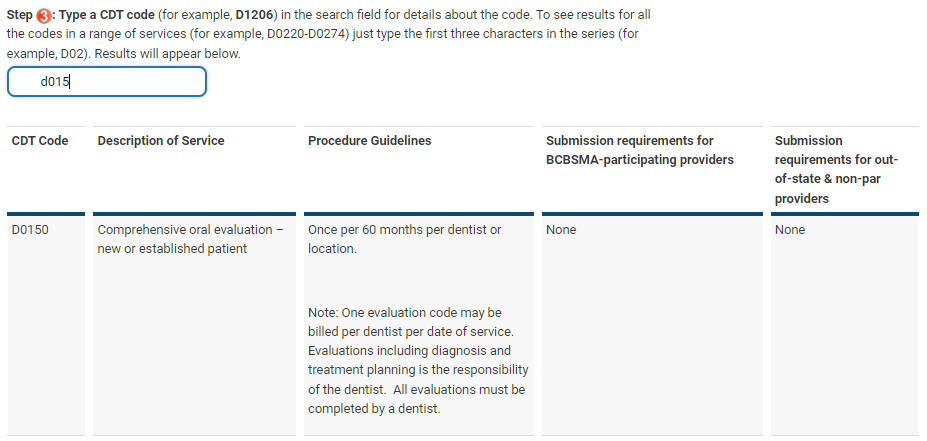
For members covered under our Pediatric Essential dental plans, your results will look like this:
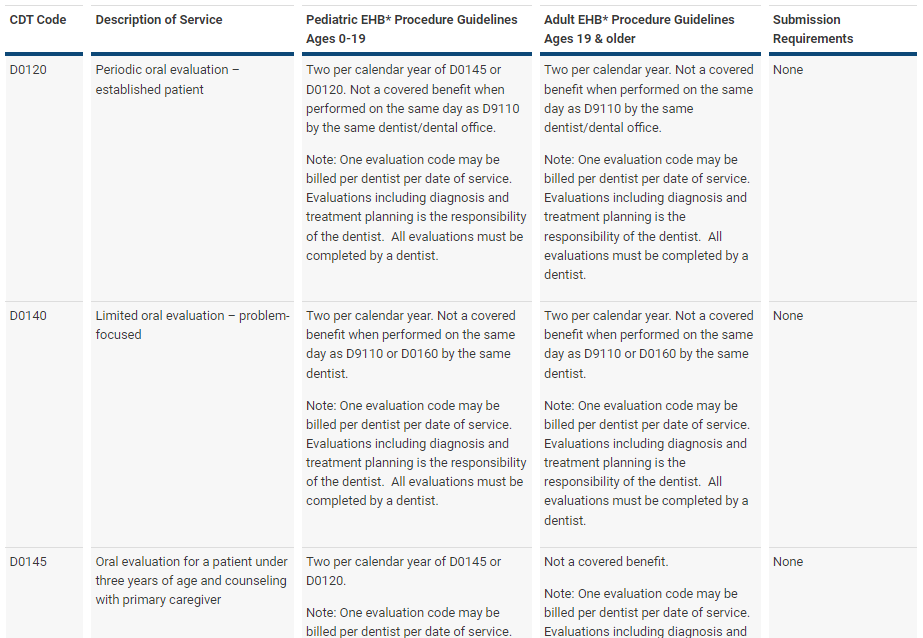
MPC_011223-2K-2-ART
This article is for acute care hospitals caring for our members
Effective April 1, 2022, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_111521-4P-6-ART
This article is for acute care hospitals caring for our members
Effective April 1, 2023, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
As always, thank you for the care you provide to your patients—our members.
Effective April 1, 2023, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
This article is for acute care hospitals caring for our members
Effective April 1, 2024, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee Schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_101923-1P-5-ART
This article is for acute care hospitals caring for our members
Effective for dates of service on or after April 1, 2025, we’ve updated our commercial HMO, PPO, and Indemnity hospital outpatient fee schedules in accordance with your existing provider contract to:
- Include new and unpriced Current Procedural Terminology (CPT®΄) and Healthcare Common Procedure Coding System (HCPCS) codes
- Update drug fees to reflect pricing based on current benchmarks
- Delete codes that are no longer valid
These updates enable us to maintain consistency with industry practices for billable codes and fees.
Resources
Resources
- Additions and deletions to the acute care hospital outpatient fee schedule, effective April 1, 2025
- Outpatient drug fee schedule for 2025, 2nd quarter
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
Complete electronic versions of your hospital outpatient fee schedules are available from your network representative.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE(2583). As always, thank you for the care you provide to our members.
MPC_121324-1R
Effective April 1, 2021, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly
- Pricing based on current benchmarks
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
This article is for acute care facilities caring for our members
Blue Cross reimburses for outpatient surgical services as outlined in our existing Outpatient Surgical Services – Facility payment policy. To download this policy, log in and go to Office Resources>Policies & Guidelines>Payment Policies.
As a reminder, we reimburse outpatient surgical services at a case rate, which reflects the fee for each allowable surgery, including diagnostic services directly related to the surgical procedure.
Our payment policy states that Blue Cross:
- Separately reimburses laboratory, radiology, or other diagnostic tests or procedures that are unrelated to the surgical procedure.
- Does not separately reimburse services, such as diagnostics, that are directly related to the allowable surgical procedure. Reimbursement is included as part of the surgical case rate.
Effective Q3 2023, we will process claims in accordance with our Outpatient Surgical Services — Facility payment policy.
Important billing reminders
Be sure to bill:
- CPT and HCPCS codes with the appropriate revenue code to trigger the correct surgical case rate.
- Facility services administered on the day of the surgery on the same claim form to ensure accurate reimbursement.
- Multiple surgeries on the same claim form with the appropriate revenue codes and corresponding valid CPT or HCPCS surgical procedure codes.
See our Outpatient Surgical Services – Facility payment policy for additional billing guidelines.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_071223-1P-1
This article is for acute care facilities caring for our members
Blue Cross reimburses for outpatient surgical services as outlined in our existing Outpatient Surgical Services – Facility payment policy.
As a reminder, we reimburse outpatient surgical services at a case rate, which reflects the fee for each allowable surgery and services considered included in the allowable reimbursement.
Our current payment policy states that Blue Cross:
- Separately reimburses laboratory, radiology, or other diagnostic tests or procedures that are unrelated to the surgical procedure.
- Does not separately reimburse services considered included in the surgical case rate, such as:
- Primary surgical dressings, supplies, splints, casts, appliances, and other equipment directly related to the performance of the surgical procedure.
- Please see our Outpatient Surgical Services – Facility payment policy for additional examples of services included in the allowable reimbursement.
As of Q2 2024, services that are not separately reimbursable from the surgical case rate will process in accordance with our existing payment policy. This will help reduce the number of claims that will require a post-payment review.
Important billing reminders
Be sure to bill:
- CPT and HCPCS codes with the appropriate revenue code to trigger the correct surgical case rate.
- Facility services administered on the day of the surgery on the same claim form to ensure accurate reimbursement.
- Multiple surgeries on the same claim form with the appropriate revenue codes and corresponding valid CPT or HCPCS surgical procedure codes.
See our Outpatient Surgical Services – Facility payment policy for additional billing guidelines.
To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_071223-1P-2
This article is for all medical and mental health providers who have a direct connection to Change Healthcare
In June, we instituted a temporary waiver for timely filing of claims in response to the Change Healthcare cybersecurity event.
For claims submitted on or after December 1, 2024, we will resume our standard filing guidelines for provider submitted claims. This will apply to our commercial, Medicare Advantage, and Federal Employee Program plans as follows:
- Claims must be filed within 90 days of the date of service.
- Appeals must be submitted within one year of the date the claim denied.
Resources
- Timely Filing Guidelines on Provider Central
- Change Healthcare Event page
Thank you
Thank you for submitting your claims within the required timeframes.
MPC_022224_1J-24
This article is for dentists caring for our members
For practices that have more than one location, please be sure to submit the rendering/treating provider’s address. This will help your claim process more accurately. Here’s how:
| For this type of claim | Please |
|---|---|
| Electronic |
Complete the following fields:
|
| Paper |
Complete box 56 along with the other fields listed within the “Treating Dentist and Treatment Location Information” section as shown below.
Populate box 49 with the group NPI and billing address. |
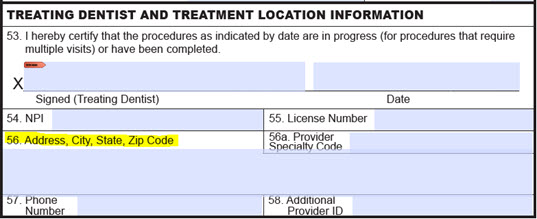
MPC_010323-1P-7
As a reminder, our temporary COVID-19 payment policy includes telehealth and online digital codes that apply to Federal Employee Program (FEP) and Medicare Advantage products only.
Please review the “Telehealth and telephonic services” section in the temporary COVID-19 payment policy to see these codes.
You can also access this information on your fee schedule by logging in and going to Office Resources>Billing & Reimbursement>Fee Schedules.
Resources
Questions?
Call Network Management and Credentialing Services at 1-800-316-BLUE (2583).
This article is for all providers caring for our members
Consistent with the CPT definition of the telephonic codes 98966-98968 and 99441-99443 and with certain telehealth codes, Blue Cross Blue Shield of Massachusetts will not reimburse for these services when a related evaluation and management (E/M) service has been provided:
- Within the previous seven days, or
- When it leads to an E/M service or procedure within the next 24 hours
Blue Cross will begin enforcing the CPT code descriptions on April 1, 2021.
- Do not report these codes if the service is related to the E/M service provided within the timeframes outlined in the code definition.
- Report these codes if the service is not related to an E/M service provided within the timeframes outlined in the code definition.
For billing information, please refer to the code descriptions and examples below.
Examples
Scenario 1: Billing a telephonic code inappropriately
- A patient is seen on April 1, 2021 for an established patient visit, and E/M code 99213 is billed.
- A telephone call related to the April 1 visit occurs between the patient and the provider on April 5, 2021.
The telephone visit should not be reported because it is within the timeframe and related to the original visit. We will only reimburse the established patient visit E/M code 99213.
Scenario 2: Billing a telephonic code appropriately
- A patient is seen on May 1, 2021 for an established patient visit, and E/M code 99213 is billed.
- On May 25, 2021, the patient and the provider have a telephone call.
The telephone visit should be reported. We will reimburse both the established patient visit E/M code 99213 and the telephone visit CPT, regardless of whether the visits were related. This is because the two visits were not within the same seven-day timeframe.
The list of codes below is included for informational purposes only. This is not a complete list of all the codes containing the CPT code descriptions outlined above. Whether or not a code is listed here does not guarantee coverage or reimbursement.
| Code | Description |
|---|---|
| 98966 | Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous 7 days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion |
| 98967 | Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous 7 days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 11-20 minutes of medical discussion |
| 98968 | Telephone assessment and management service provided by a qualified nonphysician health care professional to an established patient, parent, or guardian not originating from a related assessment and management service provided within the previous 7 days nor leading to an assessment and management service or procedure within the next 24 hours or soonest available appointment; 21-30 minutes of medical discussion |
| 99441 | Telephone evaluation and management service by a physician or other qualified health care professional who may report evaluation and management services provided to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion |
| 99442 | Telephone evaluation and management service by a physician or other qualified health care professional who may report evaluation and management services provided to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 11-20 minutes of medical discussion |
| 99443 | Telephone evaluation and management service by a physician or other qualified health care professional who may report evaluation and management services provided to an established patient, parent, or guardian not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 21-30 minutes of medical discussion |
Resources
- Frequency Payment Policy (log in and go to Office Resources>Policies and Guidelines>Payment Policies)
- COVID-19 Temporary Payment Policy
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you give to your patients—our members.
MPC_012221-1Z
This article is for acute care hospitals caring for our members
Effective July 1, 2022, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_111521-4P-8
This article is for acute care hospitals caring for our members
Effective July 1, 2023, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
As always, thank you for the care you provide to your patients—our members.
Effective July 1, 2023, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_120922-2H-7
This article is for acute care hospitals caring for our members
Effective July 1, 2024, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee Schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_101923-1P-5-ART
Effective July 1, 2020, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_111819-4W-6
Effective July 1, 2021, we have updated our commercial HMO, PPO, and Indemnity hospital outpatient drug fee schedules to include:
- New drug CPT and HCPCS codes released quarterly.
- Pricing based on current benchmarks.
These updates enable us to maintain consistency with industry practices for billable drug codes and fees.
To download your fee schedules, log in and go to Office Resources>Billing & Reimbursement>Fee schedules.
As always, thank you for the care you provide to your patients—our members.
MPC_113020-1K-8
This article is for acute care hospitals, orthopedists, rheumatologists, and physical medicine and rehabilitation physicians who administer trigger point injections
Blue Cross covers trigger point injections for the treatment of myofascial pain syndrome as outlined in our existing medical policy, Trigger Point and Tender Point Injections, 604. As a reminder, there are several statements in the policy that describe conditions that must be met for the listed codes to be covered for our commercial members:
- There is a regional pain complaint in the expected distribution of referral pain from a trigger point, AND
- There is spot tenderness in a palpable taut band in a muscle, AND
- There is restricted range of motion, AND
- Conservative therapy (for example, physical therapy, active exercises, ultrasound, heating or cooling, massage, activity modification, or pharmacotherapy) for six weeks has failed or is not feasible, AND
- Trigger point injections are provided as a component of a comprehensive therapy program, AND
- No more than four injections are given in a 12-month period.
Medical policy application
- Enforcement of this medical policy occurs through system edits and post-payment reviews.
- We continually expand our ability to process claims in accordance with this policy before we reimburse you, which will reduce the number of claims we review post-payment.
Resources
The included codes and diagnoses are listed on the Trigger Point and Tender Point Injections medical policy, which will be updated on our website on September 1.
MPC_071921-3T-1-ART
This article is for anesthesiologists and gastroenterologists caring for our members
Effective for dates of service on or after July 1, 2023, we will implement diagnosis-driven claim edits to reinforce our existing medical policy 154 guidelines. As a reminder, we cover monitored anesthesia care (MAC) for endoscopic procedures such as colonoscopies and upper endoscopies when medically necessary. Medical policy 154 describes clinical scenarios where monitored anesthesia care is medically necessary for endoscopic procedures, outlined by certain medical conditions and complication risks.
Our medical policy aligns with the American Society of Gastrointestinal Endoscopy (ASGE), American College of Gastroenterology, American Gastroenterological Association, and American Society of Anesthesiologists (ASA) guidelines.
Why are we doing this?
- In accordance with the above guidelines, endoscopic procedures can be performed under either moderate sedation or monitored anesthesia care.
- In appropriately selected patients, moderate sedation is comparably safe and more cost effective than monitored anesthesia care.
- The member’s cost share is the same for either monitored anesthesia care or moderate sedation, and the amount is based on their plan benefits.
- Note: If an endoscopic procedure is performed under monitored anesthesia care and does not align with medical policy 154, the member is not liable for the non-covered amount.
As a result of processing claims in accordance with our policy on a pre-payment basis, we are able to reduce the number of claims needing post-payment review.
Resources
![]() Medical policy 154 - Monitored Anesthesia
Care (MAC)
Medical policy 154 - Monitored Anesthesia
Care (MAC)
MPC_120522-1Q-1
Blue Cross Blue Shield of Massachusetts covers electrical stimulation of the spine devices as described in medical policy 498: Electrical Stimulation of the Spine as an Adjunct to Spinal Fusion Procedures. As previously announced, we're updating this medical policy, effective November 14, 2022, to further clarify which diagnoses we cover for these services.
| Policy change summary | Effective date | Products affected | Provider actions required |
|---|---|---|---|
| Enforcement update. Diagnoses codes list added. New diagnoses-to-CPT codes edit implemented. Policy criteria unchanged. |
November 14, 2022 | Commercial | No action required. |
As a reminder, the medical policy describes conditions that must be met for the device to be covered for our commercial members.
Additional information
- We are updating our claim system to reflect the covered diagnoses included in the policy. This helps reduce claims we review after they’ve processed and paid.
MPC_101122-4G-1


