We want you to know that the following information is available on our website.
| Programs & guidelines | To learn more, go to |
|---|---|
| Health management programs Resources about case management, care management for chronic conditions, and referrals. |
Health Management Programs |
|
Member rights and responsibilities
Information about access-to-care and member rights and responsibilities. |
Medicare Advantage Member Policies and Procedures Office Resources>Policies & Guidelines>Provider Manuals See Member Rights and Responsibilities |
About our utilization management standards
As part of our compliance with NCQA, we want providers to understand our standards for utilization management.
- We encourage appropriate use and discourage over- and under-use of health care services.
- We do not reward or offer financial incentives to utilization management staff to encourage decisions that result in under-utilization of care.
- We do not specifically reward practitioners or other individuals for issuing denials of coverage.
- We do not incentivize or encourage barriers to care and service.
- Utilization management decision-making is based only on appropriateness of care and service and existence of coverage.
MPC_012621-2Y-1–ART
We want you to know that the following information is available on our website.
| Programs & guidelines | To learn more, go to |
|---|---|
| Health management programs
Resources about case management, care management for chronic conditions, and referrals. |
Health Management Programs |
|
Member rights and responsibilities
Information about access-to-care and member rights and responsibilities. |
Medicare Advantage Member Policies and Procedures Office Resources>Policies & Guidelines>Provider Manuals See Member Rights and Responsibilities To get a paper copy, please call us at 1-800-882-2060. |
About our utilization management standards
As part of our compliance with NCQA, we want providers to understand our standards for utilization management.
- We encourage appropriate use and discourage over- and under-use of health care services.
- We do not reward or offer financial incentives to utilization management staff to encourage decisions that result in under-utilization of care.
- We do not specifically reward practitioners or other individuals for issuing denials of coverage.
- We do not incentivize or encourage barriers to care and service.
- Utilization management decision-making is based only on appropriateness of care and service and existence of coverage.
MPC_012621-2Y-1–ART
We want you to know that the following information is available on our website.
We want you to know that the following information is available on our website.
| Programs & guidelines |
To learn more, go to |
|---|---|
|
Health management programs |
|
|
Member rights and responsibilities Information about access-to-care and member rights and responsibilities. |
Log in and go to Office Resources>Policies & Guidelines>Provider Manuals
|
About our utilization management standards
As part of our compliance with NCQA, we want providers to understand our standards for utilization management.
- We encourage appropriate use and discourage over- and under-use of health care services.
- We do not reward or offer financial incentives to utilization management staff to encourage decisions that result in under-utilization of care.
- We do not specifically reward practitioners or other individuals for issuing denials of coverage.
- We do not incentivize or encourage barriers to care and service.
- Utilization management decision-making is based only on appropriateness of care and service and existence of coverage.
MPC_052523-3K-1-ART
AcariaHealth Fertility is leaving our fertility specialty pharmacy network1, 2 as of August 31, 2020. Please start directing members to one of these other specialty pharmacies in our network for fertility specialty medications:
| Name of pharmacy | Contact information |
|---|---|
| Freedom Fertility Pharmacy | Phone: 1-866-297-9452 Fax: 1-888-660-4283 www.freedomfertility.com |
| Metro Drugs | Phone: 1-888-258-0106 Fax: 1-201-253-1101 www.metrodrugs.com |
| Village Fertility Pharmacy | Phone: 1-877-334-1610 Fax: 1-877-334-1602 villagepharmacy.com |
What happens to members currently using AcariaHealth Fertility?
We’ll notify members about this change, so they can switch to an in-network specialty pharmacy.
Resources
Specialty Pharmacy
![]() Blue
Cross Blue Shield of Massachusetts Formulary: Specialty Pharmacy
Medications (we’ll update this list to remove AcariaHealth Fertility).
Blue
Cross Blue Shield of Massachusetts Formulary: Specialty Pharmacy
Medications (we’ll update this list to remove AcariaHealth Fertility).
- Members who have our Blue Cross standard formulary and members who use the National Preferred Formulary are required to fill specialty medications through an in-network specialty pharmacy.
- AcariaHealth will remain in our specialty pharmacy network for non-fertility specialty medications.
MPC_021419-1F-11
AcariaHealth is leaving our specialty pharmacy network1 as of July 1, 2024.
Please start directing members to one of these other specialty pharmacies in our network for specialty medications.
| Name of pharmacy: | Contact information: |
|---|---|
| Accredo Health Group | Phone: 1-800-987-4904 option 5 Fax: 1-800-391-9707 accredo.com |
| AllianceRx Walgreens Pharmacy (To be known as Walgreens Specialty Pharmacy as of August 1, 2024) |
Phone: 1-888-347-3416 Fax: 1-877-231-8302 AllianceRxwp.com/specialty-pharmacy |
| CVS Specialty | Phone: 1-866-846-3096 Fax: 1-800-323-2445 cvsspecialty.com |
What happens to members currently using AcariaHealth?
We’ll notify members about this change, so they can switch to an in-network specialty pharmacy.
Resources
- Specialty Pharmacy page
- Specialty Pharmacy Medication List
(we’ll update this list on July 1, 2024 to remove AcariaHealth and on August 1 for Walgreens Specialty Pharmacy).
- Members who have our Blue Cross Blue Shield of Massachusetts formulary and members who use the Standard Control with Advanced Control Specialty Formulary (managed by CVS Caremark) are required to fill specialty medications through an in-network specialty pharmacy.
MPC_041724-2
This article is for providers who order vitamin D testing and clinical and hospital laboratories that conduct the tests.
We recently announced updates to our medical policies that will take effect December 1, 2019. We want to share additional details about changes to Testing Serum Vitamin D Levels Medical Policy 746, so our members receive the recommended testing.

We’ll use the same diagnoses as CMS to determine medical necessity
Starting on December 1, 2019, when determining coverage for testing vitamin D deficiency, we will use the same diagnoses that the Centers for Medicare & Medicaid Services (CMS) uses. Please refer to Local Coverage Determination ID L37535: Vitamin D Assay Testing for the list of diagnosis codes.
Coverage for these diagnoses will apply to our commercial (HMO/POS and PPO) and indemnity members when the service is billed with:
- CPT 82306: Vitamin D; 25 hydroxy, includes fraction(s), if performed
- CPT 82652: Vitamin D; 1, 25 dihydroxy, includes fraction(s), if performed
We already use CMS’ local coverage determination criteria for our Medicare Advantage members.
What happens if the claim submitted does not include the diagnosis code?
If the claim for the CPT code does not have a covered diagnosis code, the claim will deny for not meeting medical policy guidelines.
Why is Blue Cross making this change?
Research suggests that vitamin D testing is often unnecessarily ordered for patients who aren’t at risk. For example, the US Preventive Services Task Force concludes that, “the current evidence is insufficient to assess the balance of benefits and harms of screening for vitamin D deficiency in asymptomatic adults.”
Member resource
The Choosing Wisely website offers a downloadable PDF that you can share with patients to describe when vitamin D deficiency screening may be needed.
Thank you
Thank you for helping our members to receive tests that are clinically effective.
MPC_070819-1Y-1-ART
This article is for:
- Home health care providers
- Mental health clinicians
- Providers who recommend home health care services to our members

We recently announced that we have eliminated authorization requirements for home health care services for our commercial members. This is intended to ease administrative burden and provide quick access to our members who need home care services—especially those being discharged from an inpatient facility who want to continue treatment at home.
Here we answer questions we’ve received from home health care agencies about this announcement and share information about our home health care benefit as it relates to mental health services.
For dates of service on and after January 1, 2024:
- We no longer require a global authorization for our commercial HMO, POS, EPO, and PPO1 members. You also do not need to request authorization throughout the episode of care.
- This applies to home health care services provided by an in-network agency, such as skilled nursing care; physical, occupational and speech therapy; social work; and home health aide services.
- You don’t need to add an authorization number to your claims. Our claims system will process the claim by the date of service. If you need a retroactive authorization for a service before December 31, 2023, please call us at 1-800-327-6716 or fax the request to 1-888-282-0780.
1 Federal Employee Program members already do not require authorization.
We continue to require authorization for:
- Medicare HMO Blue members. Please follow your existing processes for Medicare HMO Blue members.
- Home infusion therapy services for all members.
- Private duty nursing for plans that offer this benefit.
We don’t require referrals for home health care services. Orders can be written by the member's treating provider—PCP, psychiatrist, or other specialty.
Use an online tool, such as ConnectCenter, to check member benefits and eligibility.
If you’d like to see if the member has a benefit maximum for home health care services, see our ConnectCenter Quick Start Guide (screenshot below) for instructions.
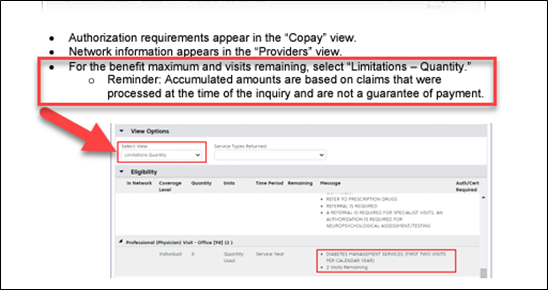
For commercial members, we use InterQual®' criteria to determine medical necessity. To access the InterQual criteria, you’ll need to log on to Provider Central and navigate to Clinical Resources>InterQual Criteria. Click the “Go now” button and select “LOC: Home Care Q & A” to access them.
For commercial members, we use InterQual®' criteria to determine medical necessity.
For Medicare Advantage members, we use CMS’ criteria.
Keep in mind that members with mental health conditions may qualify for home health care services, just as members with physical conditions do. For example, patients may be eligible for home health services if they are recently discharged from an inpatient stay at an acute care hospital or a behavioral health hospital and need medication administration support for injectable medications.
Here's how this might work:
- An HMO member needs psychiatric care.
- If the psychiatrist determines that the patient needs home health care (for example, to help them inject their medication), the psychiatrist’s office would coordinate the care with the home health care organization.
- The home health care agency will need doctor's orders from the psychiatrist.
- No global authorization is required.
Resources
- Home health care page
- InterQual Criteria
- InterQual Criteria (log in required)
- ConnectCenter: For member eligibility and benefits verification, claim status, and more. You’ll find tips, resources, and other information to help support your use of the tool
- Authorization Manager: To check authorization requirements
MPC_091923-2Y-3-ART
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in April 2020 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates, grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in April 2021 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in April 2022 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in April 2023 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in April 2024 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
This article is for physicians, clinicians, and their office staff who order:
- Vitamin B-12 testing
- Respiratory pathogen panels
And for clinical and hospital laboratories that conduct these tests.
Please share with your biller or billing agency.
In September, we notified you of medical policy changes that will take effect on December 1, 2023. We’re reminding you of these changes so our members receive the recommended testing.
- Vitamin B-12 Testing medical policy 061 (new policy)
- Pathogen Panel Testing medical policy 045 (revised policy)

Medical necessity is based on a covered diagnosis
The tests listed below aren’t covered routinely. Members must have a diagnosis that is listed in our medical policy for us to consider the tests medically necessary. If a claim is submitted for one of the tests and includes a non-covered diagnosis, the claim will deny.
Criteria and diagnosis codes
|
Type of test |
Is considered medically necessary | You can find covered diagnosis codes by |
|---|---|---|
| Vitamin B-12 testing |
For commercial and Medicare Advantage members with these conditions:
|
Referring to Vitamin B-12
Testing medical policy 061. Note: This policy will be posted on December 1, 2023. |
| Respiratory pathogen panel tests |
For commercial members with these conditions when the panel has:
For Medicare Advantage members, we already use CMS’ local coverage determination criteria. |
Referring to Pathogen Panel Testing medical policy 045. Note: This revised policy will be posted on December 1, 2023. |
Thank you
Thank you for helping our members to avoid additional costs by ordering covered tests.
MPC_090723-1P-1

Mental health issues have become increasingly prominent due to the pandemic, with more people having developed debilitating conditions such as depression and anxiety. Despite this, it can be difficult to identify symptoms in otherwise healthy patients.
Stephanie Hansbury, a mom of two, recently recovered from breast cancer. Although she was physically healthy once cancer-free, the taxing series of treatments took a heavy toll on her mental health. Read our Coverage article to see how therapy and antidepressants helped her recover from major depression.
In a recent survey of our mental health providers, we found that less than half regularly collaborate with their patients’ medical providers. Studies have shown that a comprehensive approach to care, one that addresses both medical and mental health, leads to better outcomes and an improved patient experience.
For patients with medical and mental health comorbidities, collaboration among their healthcare team results in:
- Fewer complications with treatment and prescribed medications
- Higher patient satisfaction
- Less burden on the patient to manage their own care
- Lower readmission rates
- More coordinated continuity of care
It’s evident that primary care providers (PCPs) and mental health clinicians can help their patients achieve better health outcomes by working in tandem. While both have key roles in this joint effort, PCPs should be empowered to take the lead.
A common barrier for PCPs is having access to mental health consultants. Ashley Yeats, MD, a board-certified family physician and vice president of medical operations at Blue Cross Blue Shield of Massachusetts, states, “That’s why Blue Cross has expanded access to mental health providers who leverage telehealth. We’re excited to widen our network, contracting with practices such as Thriveworks, Headway, Refresh Mental Health, and Valera Health. These providers offer mental health telehealth services and can support the delivery of PCP-led, comprehensive primary care.” Roughly 69 percent of our members find it important to have both telehealth and in-person care options, which these new partners offer.
Medical and mental health providers both play vital roles in solving the coordination of care puzzle. Once a patient is established with a mental health professional, collaboration between the medical and mental health providers should occur when appropriate. This ensures that the patient has a cohesive treatment plan that addresses both the mind and body. “As a PCP taking the lead, you can create a seamless and integrated experience for your patient,” said Yeats.
As always, thank you for the care you provide to our members.
MPC_060822-3M-1-ART
This article is for primary care providers caring for our Medicare Advantage members
This week, we’ll begin sending letters to our Medicare Advantage members who may be due for a colorectal cancer screening to let them know that they’re eligible to receive a Cologuard® kit. Cologuard is a covered, non-invasive screening option that members can complete from the comfort of their home, and is available at $0 copay.
Who is eligible for Cologuard?
Using our claims data, we’ve identified Medicare Advantage members who appear to be due for colorectal cancer screening and may be appropriate for a Cologuard screening1. Cologuard tests are recommended every three years.
How will members receive the kit?
Members who receive the letter are prompted to call Blue Cross and speak with our Engagement Specialist to complete a brief pre-screening to ensure there is no family history or increased risk of colon cancer. Once the member passes this pre-screening, we’ll share their information with Exact Sciences, an independent health screening organization, who will then ship the Cologuard kit2.
If the member does present an increased risk, we’ll point them back to you to review all screening options that are available to them.
How will I get the results?
Exact Sciences will mail results to the member within two weeks after receiving the Cologuard sample. If the member has identified you as their PCP, Exact Sciences will automatically share results with you.
See what we’re sending to members
1INDICATIONS AND IMPORTANT RISK INFORMATION: Cologuard is intended to screen adults 45 years of age and older who are at average risk for colorectal cancer by detecting certain DNA markers and blood in the stool. Cologuard is not a replacement for colonoscopy in high-risk patients. Patients with a positive test result should be referred for colonoscopy. A negative test result does not confirm the absence of cancer. Patients with a negative test result should discuss with their doctor when they need to be tested again.
2 We’re working with Exact Sciences and LifeLine Community Healthcare, an independent health screening organization, to send Cologuard kits to members. Cologuard is shipped through the provider, Exact Sciences who works with clinicians at LifeLine to order Cologuard for the member.
Have you seen all the patients in your panel this year? If not, now is the time to find out if they have delayed routine services and follow up to make sure they get scheduled. To help, we’re sending wellness reminders to members in August.
Who will receive reminders?
All members with asthma, coronary artery disease, or diabetes whose claims data show gaps in their care between January 1-June 30, 2022, will receive letters encouraging them to stay on track with managing their health.
- This includes members who belong to our Medicare Advantage, commercial HMO and PPO, and Federal Employee Program (FEP) health plans.
| Members who have |
Age (As of December 31, 2022) |
Will receive information about | Sample letter |
|---|---|---|---|
| Asthma |
5+ |
Medication to control asthma:
|
See samples of health and wellness reminders: |
| Coronary artery disease |
|
|
|
| Diabetes |
18+ |
|
Keep preventive care a priority for your patients
Eligible members may also receive mail, email, or text reminders about the importance of the following care:
- Cervical cancer screening (members over age 19)
- Colorectal cancer screening (members over age 46)
- Dental visit
- Breast cancer screening (members over age 52)
- Routine health checkup
You can support the health and wellness of your patients with these conditions by reinforcing these messages, scheduling preventive care appointments, and discussing at-home screening options when appropriate.
More resources for members with diabetes
This fall, we’ll also work with limited services clinics—like CVS MinuteClinic—and CVS HealthHUBTM locations in Massachusetts to offer convenient testing and screenings for our members diagnosed with diabetes. These clinics may also prescribe recommended medications. A CVS care concierge may also reach out to members to help them understand their care options.
Because we recognize the importance of the patient-provider relationship, we’ll steer members back to you—their PCPs and treating clinicians—whenever possible.
As always, thank you for the care that you give your patients—our members.
MPC_040122-1C-1
We’ve added coverage for Medicare Advantage members below. We’ve also added information on free tests from the federal government.
We’ve added a clarification for FEP member coverage below.
This article is for all providers caring for our members
As of January 15, 2022, we will cover up to eight self-administered at-home tests per commercial member per month for personal, diagnostic use, without cost and without any need for prior clinical assessment. We will also reimburse up to $12 per FDA-authorized, self-administered at-home test for up to four tests per month for Medicare Advantage members.
The coverage is not retroactive and will not apply to any test kit purchases made prior to January 15, 2022.
Eligible members can complete the COVID-19 At-Home Test Reimbursement form (PDF). Eligible Medicare Advantage members can complete the Medicare Advantage COVID-19 At-Home Test Reimbursement form (PDF).
For more information on the new policy, visit here for details.
Additionally, we will continue to cover FDA-authorized COVID diagnostic tests, such as PCR tests, with no cost share to members when ordered or administered by a health care provider following an individualized clinical assessment. This applies to our commercial and Medicare members.
For information regarding coverage for our FEP members, please visit www.fepblue.org/coronavirus-updates/over-the-counter-tests.
As of January 19, every household in the U.S. is also eligible to order up to four free, at-home COVID-19 tests from the federal government. People can order free tests here.
MPC_030620-1N-210
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in August 2020 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates, grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in August 2021 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in August 2022 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in August 2023 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
We’ve posted new, revised, clarified, and retired medical and pharmacy medical policies, effective in August 2024.
Medicare Advantage policies
![]() Medical policy
132, Medicare Advantage Management
Medical policy
132, Medicare Advantage Management
(This document explains whether we use CMS criteria—or our own—to make coverage determinations for our Medicare Advantage members.)
Medicare Advantage section of our medical policy site.
FEP medical policies
Visit fepblue.org and search for medical policies.
MPC_110215-3D
This article is for all providers caring for our members
We continue to waive authorization requirements and expedite credentialing applications through the dates listed below. This is in response to the Division of Insurance Bulletin 2022-03 – Relaxation of Prior Authorization and Credentialing Procedures in Response to Health Facility Staffing and Capacity Constraints (issued February 23, 2022).
Authorization requirements continue to be waived for Commercial HMO and PPO, and Indemnity members only for the following services:
- All inpatient treatment, both COVID-19 and non-COVID-19-related, at acute care and post-acute care facilities
- Mental health admissions
- Scheduled surgeries
Important note: Services for Medicare Advantage and Federal Employee Program (FEP) members will continue to follow standard prior authorization processes.
Continue to notify of admissions
Through dates of service up to and including May 16, 2022, inpatient acute care hospitals and mental health hospitals must continue to notify us of inpatient admissions. Timely notification serves to facilitate care coordination, mobilize services to support transition of care, and ensure prompt claims processing. While this notification-only requirement is in place, we will not perform medical necessity reviews.
Definitions
| Notification only required | Does not require submission of clinical documentation for initial admission or concurrent review |
| Medical necessity review required | Requires that the requesting provider submit clinical documentation in support of the request |
Notification requirements by service and product
These requirements are in effect for dates of service through May 16, 2022.
| Level of care or service | Requirement for Commercial HMO and PPO; Indemnity |
|---|---|
| Behavioral health – inpatient | Notification only |
| Behavioral health – acute residential treatment (partial hospitalization & intensive outpatient program) | Notification only |
| Pre-service inpatient (For dates of service on or before May 16, 2022) |
Notification only |
| Skilled nursing facility, rehabilitation, and long-term acute care hospitals Benefit limits still apply |
Notification only |
| Home health care Benefit limits still apply |
Medical necessity review |
Concurrent and retrospective reviews
Beginning April 18, 2022, we will resume concurrent and retrospective reviews of the first five days of any post-acute facility stay following a transfer from an acute or mental health hospital. Until then, we are conducting concurrent review at day six.
Postponed procedures
If you previously received an approved authorization for a service that was postponed, please be sure to notify us if you have a new date. This will help with claim processing.
Expediting credentialing
We will expedite credentialing for all new providers and for all credentialing applications in process to meet the recent DOI guidance. You do not need to do anything. We will confirm your approval and effective date through our standard correspondence.
MPC_111921-1Q-2-ART
This article is for all providers except dentists
As of June 30, 2021, Authorization Manager will allow requesters to complete the InterQual® medical necessity checklist for certain procedures performed in an outpatient setting.
What services are included?
- Back surgery
- Hip surgery
- Knee surgery
- Hysterectomy
How does this increased functionality work?
- The user initiates initial review request in Authorization Manager.
- If a CPT code for back, hip, knee, or hysterectomy surgery is entered, the user will be routed to InterQual.
- The InterQual criteria will display in a checklist format. The user will make selections based on the patient’s known symptoms, diagnostic testing, and prior treatments.
- If InterQual criteria are met and member’s eligibility is active, the authorization will be approved automatically.
If the criteria aren’t met, or the code entered is not associated with these services, the authorization will pend for manual review and you will be notified.
Resource
![]() Launch InterQual from Authorization Manager fact sheet
Launch InterQual from Authorization Manager fact sheet
MPC_012618-1L-65
This article is for all providers caring for our members
To address health facility staffing and capacity constraints, effective as of November 18, 2021, we are waiving authorization requirements and expediting credentialing applications through February 15, 2022. This is in response to the Division of Insurance Bulletin 2021-15 – Relaxation of Prior Authorization and Credentialing Procedures in Response to Health Facility Staffing and Capacity Constraints.
Authorization requirements are waived for Commercial HMO and PPO, and Indemnity members only for the following services:
- All inpatient treatment, both COVID-19 and non-COVID-19-related, at acute care and post-acute care facilities
- Mental health admissions
- Scheduled surgeries
Important note: Services for Medicare Advantage and Federal Employee Program (FEP) members will continue to follow standard prior authorization processes.
Continue to notify of admissions
Through dates of service up to and including February 15, 2022, inpatient acute care hospitals and mental health hospitals must continue to notify us of inpatient admissions. Timely notification serves to facilitate care coordination, mobilize services to support transition of care, and ensure prompt claims processing. While this notification-only requirement is in place, we will not perform medical necessity reviews.
Definitions
| Notification only required | Does not require submission of clinical documentation for initial admission or concurrent review |
| Medical necessity review required | Requires that the requesting provider submit clinical documentation in support of the request |
Notification requirements by service and product
These requirements are in effect for dates of service through February 15, 2022.
| Level of care or service | Requirement for Commercial HMO and PPO; Indemnity |
|---|---|
| Behavioral health – inpatient | Notification only |
| Behavioral health – acute residential treatment (partial hospitalization & intensive outpatient program) | Notification only |
| Pre-service inpatient (For dates of service on or before February 15, 2022) |
Notification only |
| Skilled nursing facility, rehabilitation, and long-term acute care hospitals Benefit limits still apply |
Notification only |
| Home health care Benefit limits still apply |
Medical necessity review |
Delaying authorization requirements for commercial EPO, PPO (not for Medicare Advantage)
We previously notified you that we would require prior authorization for services listed in our medical policies for EPO, PPO, and Medicare Advantage members, including:
- Continuous glucose monitors
- Other services
Given the guidance from the DOI, we will only require prior authorization for Medicare Advantage members starting on January 1, 2022.
Expediting credentialing
We are also expediting credentialing for providers to meet the recent DOI requirement.
What does this mean if you are going through credentialing now or if it’s in process?
You do not need to do anything. We will expedite credentialing for all new providers and for all credentialing applications in process. We will confirm your approval and effective date through our standard correspondence.
MPC_111921-1Q-1
This article is for all providers caring for our members
In March, we told you that prior authorization requirements for certain services were relaxed through May 16, 2022 as required by the Division of Insurance (Bulletin 2022-03).
Effective for dates of service on and after May 17, 2022, we will resume our standard notification, prior authorization, and authorization requirements for coverage for the following services:
- All inpatient treatment, both COVID-19 and non-COVID-19-related, at acute care and post-acute care facilities
- Mental health admissions
- Scheduled surgeries
This applies to members belonging to all of our health plans, including commercial HMO, PPO, and Indemnity.
Note: We did not waive authorization requirements for Medicare Advantage or Federal Employee Program (FEP) to begin with, so standard processes continue to apply.
Notification requirements resume
We’re also resuming our usual notification and medical necessity review requirements for the following:
| Level of care or service |
|---|
| Behavioral health – inpatient |
| Behavioral health – acute residential treatment, partial hospitalization, and intensive outpatient program |
| Pre-service inpatient |
| Skilled nursing facility, rehabilitation, and long-term acute care hospitals Benefit limits still apply |
| Home health care Benefit limits still apply |
Resources
- Authorization Quick Tip
- Prior authorization overview
- Behavioral Health authorization requirements
- Authorization Manager
MPC_030620-1N-231-ART
This article is for providers caring for our members
We’re expanding prior authorization requirements for certain services listed in our medical policies to members in our commercial EPO and PPO plans as of June 1, 2022. These requirements will align with those currently in place for our commercial HMO and POS members.
Commercial EPO and PPO plan members who are:
- Currently using a service listed below and need an approved authorization for continued coverage on or after June 1, 2022
- Receiving the service on or after June 1, 2022
We’ll accept prior authorization requests up to 30 days before June 1, 2022, so that you can have an approved authorization for any services taking place after the effective date.
We previously communicated this change last September and delayed the effective date until this June.
| For these services | Please request authorization | ||
|---|---|---|---|
| Continuous glucose monitors (Codes: A9277, K0553, S1036) |
Following the same method you use today for HMO/POS members. Remember: Authorization is required on an annual basis. |
||
Spine surgeries using InterQual SmartSheets for:
|
Following the same method you use today for HMO/POS members. |
||
| Other services (refer to list of codes) | Following the same method you use today for HMO/POS members. |
As always, we recommend checking member benefits and eligibility to determine any authorization requirements. You can use Authorization Manager, available on Provider Central, to check any authorization requirements by entering the procedure code.
You can learn more about how to request authorization on our Authorization Manager page (scroll to our Guides and video demonstrations section) or view our Authorization Manager User Guide.
These resources are available and will be updated on June 1, 2022 to reflect the new authorization requirements:
- If you have questions about whether a service requires prior authorization, use Authorization Manager to look it up by CPT or HCPCS code first.
- If you aren’t able to get the information using Authorization Manager, you may call Clinical Intake at 1-800-327-6716.
As always, thank you for the care you provide to our members.
MPC_010621-1V-9
Please share with your billing department or billing agency
We made updates to our medical policies for dates of service starting on March 1, 20241. These updates may affect your authorization requests and claims for the medications below that you buy and bill to us (medical benefit medications).
 What you need to know
What you need to know
For the medications below, we’ve highlighted new steps to take when requesting authorization and submitting claims:
- Request authorization for the medication, just as you currently do.
- New: Include the dose and frequency of administration with your request.
Exception: Somatuline Depot (lanreotide) does not require prior authorization, but dosing limits will now apply to claims.
- We’ll review the authorization request.
- New: If the dose and frequency you requested is in line with our medical policy or FDA-approved dosing limits, we may approve the request. If the dose and frequency are over the limit, the authorization request will deny. If you disagree with the decision, you can always request an appeal.
- If the submitted claim matches what’s been approved, your claim will process.
- New: If it does not match what’s been approved, the claim will deny in its entirety.
- If the member had an existing authorization for the medication (prior to March 1), then the dosing and frequency edits will apply when a new authorization is requested.
Medications with dosing and frequency limits
| Name of medication | HCPCS code(s) | Medical policy |
|---|---|---|
| Actemra (Tocilizumab) | J3262 | Immune Modulating Drugs medical policy 004 |
| Avsola, Inflectra, Renflexis, Remicade | J1745, Q5103, Q5104, Q5121 | |
| Orencia (Abatacept) | J0129 | |
| Eylea (Aflibercept) | J0178 | Vascular Endothelial Growth Factor (VEGF) Inhibitors Step Therapy medical policy 092 |
| Prolia, Xgeva (Denosumab) | J0897 | Medical Utilization Management (MED UM) & Pharmacy Prior Authorization Policy 033 |
| Tepezza (Teprotumumab) | J3241 | |
| Soliris (Eculizumab) | J1300 | Soliris, Ultomiris, Myasthenia Gravis, and Neuromyelitis Optica Policy 093 |
| Lanreotide (Somatuline Depot) | J1930 | N/A |
| Xolair (Omalizumab) | J2357 |
Injectable Asthma
Medications policy 017
New: This policy update will now take effect for dates of service on and after July 1, 2024, not on March 1 as previously communicated. |
| Riabni, Ruxience, Rituxan, Truxima | J9312, Q5115, Q5119, Q5123 | Nononcologic Uses of Rituximab medical policy 123 |
| Entyvio (Vedolizumab) | J3380 | Entyvio (Vedolizumab) Policy 162 |
Resource
News Alert: Medication claim edits and medical policy updates delayed
Note: To access this News Alert, log in and go to News. Look for the News Alert from November 30, 2023 titled, Medication claim edits and medical policy updates delayed.
Questions
If you have any questions, please call Pharmacy Operations at 1-800-366-7778. As always, thank you for the care you provide to our members.
1. The Xolair (Omalizumab) policy changes will now be effective on July 1, 2024.
MPC_071823-2K-42
This article is for all providers caring for our members
According to the latest Commonwealth of Massachusetts Department of Public Health guidance, for patients for whom current preferred antiviral treatments (nirmatrevlivr/ritonavir or remdesevir) aren’t appropriate or available, the preferred monoclonal antibody treatment is Bebtelovimab.
Laboratory data has shown Bebtelovimab retains efficacy with a broad range of COVID variants, including Omicron BA.2, which is now dominant in Massachusetts. Bebtelovimab is a newer antibody treatment with emergency use authorization to be given by IV within 7 days of a patient’s first COVID symptoms.
More information
- MA Department of Public Health: Clinical Guidance on Therapeutics for COVID-19 Issued March 25, 2022
- Provider Central: COVID-19 treatments available across Massachusetts
- Coverage health news site: What you should know about COVID treatments
MPC_030620-1N-230
This article is for the mental health and primary care providers who care for our members
Starting March 31, 2024, Blue Cross will cover an annual mental health wellness exam as required by the Addressing Barriers to Care Act (ABC Act) to improve mental health care across Massachusetts. This exam may be conducted as part of the annual preventive visit with a primary care provider (PCP), or as a standalone visit with a primary care provider or licensed mental health professional.
Because the mental health wellness exam is considered preventive care, there is no out-of-pocket cost for members in most plans.
What is the mental health wellness exam?
The exam includes taking the patient’s mental health history, appropriate screening tests, shared decision-making (that could include lifestyle education and counseling) and a discussion about next steps such as referrals for treatments and medication options. The mental health wellness exam may or may not result in a diagnosis.
Who may administer the exam
- A Massachusetts licensed mental health professional
- A Massachusetts primary care provider, including OB/GYNs, as a separate exam or as part of the annual wellness visit.
How to bill for the exam
We will reimburse claims submitted with dates of service on or after March 31, 2024 that contain the following procedure and diagnosis codes. To ensure that members are not subject to out-of-pocket cost, bill with modifier 33 in the first modifier field on your claim to indicate that the evaluation is for preventive purposes.
|
Code |
Definitions and guidance |
|---|---|
|
Procedure code 90791 |
An integrated biopsychosocial assessment, including history, mental status, and recommendations |
|
Diagnosis code: Z13.30 |
Encounter for screening examination for mental health and behavioral disorders, unspecified |
Resources
For more details, please refer to:
- Our Mental Health and Substance Use payment policy. To download our payment policies, log in and click Find a Payment Policy on the right side of your home page. Or go to Office Resources>Policies & Guidelines>Payment Policies.
- The Division of Insurance Bulletin 24-02, Appendix A for mental health wellness examination criteria and guidelines based on input from medical providers convened by the Massachusetts Department of Mental Health.
For more details, please refer to our Mental Health payment policies for billing guidelines below:
- Mental Health and Substance Use
- Telehealth (Telemedicine) - Mental Health
- The Division of Insurance Bulletin 24-02, Appendix A, for mental health wellness examination criteria and guidelines based on input from medical providers convened by the Massachusetts Department of Mental Health.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to our members.
MPC_012324-2Y-1-ART
This article is for all providers caring for our members

New CMO Sandhya Rao, MD
Blue Cross Blue Shield of Massachusetts is excited to welcome Dr. Sandhya Rao as chief medical officer.
Dr. Rao comes to us from Haven, where she served as vice president of clinical strategy. Prior to that, she was senior medical director for population health management at Partners HealthCare (now known as Mass General Brigham) and associate medical director of the Mass General Physicians Organization. She received her MD from New York University. Her training in internal medicine/primary care was completed at Brigham and Women’s Hospital/Harvard Vanguard Medical Associates.
Chief Operating Officer Rich Lynch says, "Dr. Rao brings to our company qualities that are vital to our strategy and mission. Her deep clinical and health plan experience, knowledge of our state's broad provider network, exceptional population health management, and member engagement expertise, and insights into what employers want in their health plan will make her an incredibly strong asset to our company's leadership team."
Dr. Rao started at Blue Cross on December 7, 2020. She shares that, "Blue Cross has long been an innovative leader in value-based care, an advocate for universal access to quality health care, and a champion of diversity, equity, and inclusion. I am looking forward to leading a team of talented, compassionate clinicians as we face unprecedented challenges and opportunities."
MPC_122420-1W-1-ART
BriovaRx is leaving our specialty pharmacy network1 as of March 31, 2020. Please start directing members to one of these other specialty pharmacies in our network for specialty medications:
| Name of pharmacy | Contact information |
|---|---|
| AcariaHealth | Phone: 1-866-892-1202 Fax: 1-866-892-3223 www.acariahealth.com |
| Accredo Health Group | Phone: 1-800-987-4904 option 5 Fax: 1-800-391-9707 www.accredo.com |
| CVS Specialty | Phone: 1-866-846-3096 Fax: 1-800-323-2445 www.cvsspecialty.com |
What happens to members currently using BriovaRx?
We’ll notify members about this change, so they can switch to an in-network specialty pharmacy.
Note: Medicare Advantage members with a Part D prescription drug plan who use BriovaRx do not need to make any change.
Resources
- Specialty Pharmacy page
- Specialty
Medications and Pharmacy Provider Information list
(we’ll update this list on April 1, 2020 to remove BriovaRx).
- Members who have our Blue Cross standard formulary and members who use the National Preferred Formulary are required to fill specialty medications through an in-network specialty pharmacy.
MPC_021419-1F-8–ART
This article is for all providers caring for our members
The Department of Public Health (DPH) has issued a reminder to Massachusetts residents that free COVID-19 treatment options are available.* These treatments can be used to prevent severe illness and hospitalization.
There are five treatment options in Massachusetts
Oral therapy
- Molnupiravir
- Paxlovid
Monoclonal antibodies and antiviral infusion
- Bebtelovimab
- Remdesivir
- Sotrovimab
Treatments should be considered for patients with a positive COVID-19 test who are symptomatic and who are at risk for moderate-to-severe disease progression, regardless of vaccination status. For information on patient treatment qualification, read Clinical Guidance on Therapies for COVID-19.
Supply limitations are not a barrier for treatment, according to the Massachusetts Department of Public Health. Please ensure that eligible patients have access to COVID-19 therapies as soon as possible.
Treatment availability
- Oral antivirals are available at select CVS and Walgreens retail pharmacies. Patients can find treatment here: MA COVID-19 Therapeutic Locator.
- Patients can also call the COVID-19 Self-Referral Treatment Line operated by Gothams at (508) 213-1380. The Gothams call line is a free resource that can help refer individuals to sites for monoclonal antibody treatments.
Home infusion therapy providers
We encourage home infusion therapy providers to offer COVID-19 monoclonal antibody treatments and Remdesivir infusions to eligible patients in their communities.
*Anti-SARS-CoV2 monoclonal antibodies and oral antivirals are available through state-funded sites located across the Commonwealth and managed by Gothams. These state-funded infusion sites include Athol, Everett, Fall River, Holyoke, Lowell, Pittsfield, Plymouth.
MPC_030620-1N-227
Medicare sequestration also suspended through March 31
This article is for the acute care and mental health hospitals caring for our members
In September we announced that we would waive authorization requirements at inpatient acute care and mental health hospitals for dates of service through December 31, 2020.
Recognizing that hospitals continue to experience administrative resource issues due to COVID-19, we will continue to waive authorization requirements for inpatient acute care and mental health hospitals through March 31, 2021.
This extension applies to:
- All inpatient acute care and mental health admissions, whether or not related to COVID-19
- Prior authorization and concurrent reviews for inpatient admissions
- Scheduled surgeries at inpatient acute care hospitals
- All Blue Cross Blue Shield of Massachusetts products, except the Federal Employee Program (FEP). FEP follows Blue Cross Blue Shield Association referral and authorization guidelines. For more details, see fepblue.org.
Notification of admissions
Through dates of service up to and including March 31, 2021, inpatient acute care hospitals and mental health hospitals must notify us of inpatient admissions. Timely notification serves to facilitate care coordination, mobilize services to support transition of care, and ensure prompt claims processing. While this notification-only requirement is in place, we will not perform medical necessity reviews.Starting with dates of service on or after April 1, 2021, authorization requirements will be reinstated. You will need to submit requests and supporting documentation for prior authorization at that time.
Authorization requirements by service and product
These authorization requirements are in effect for dates of service through March 31, 2021.
Network requirements
All prescheduled services and admissions, including home care services and skilled nursing admissions, are expected to be referred to in-network providers. Out-of-network requests for scheduled services will be reviewed on an individual case basis.
Definitions
| Notification only required | Does not require submission of clinical documentation for initial admission or concurrent review |
| Medical necessity review required | Requires that the requesting provider submit clinical documentation in support of the request |
Authorization requirements
| Level of care or service | Commercial HMO, Indemnity, and PPO | Medicare Advantage | FEP |
|---|---|---|---|
| Behavioral health – inpatient | Notification only required | Medical necessity review required | |
| Behavioral health – acute residential treatment (partial hospitalization & intensive outpatient program) | Medical necessity review required | ||
| Behavioral health – inpatient | Notification only required | Medical necessity review required | |
| Pre-service inpatient (for dates of service on or after April 1, 2021) |
Medical necessity review required |
||
| Skilled nursing facility, rehabilitation, and long-term acute care hospitals | Notification only required (Updated January 13, 2021) |
||
| Previously approved elective surgeries | To avoid duplication of cases and ineligibility issues due to changes in member coverage since the initial approval, prior authorizations will not be automatically extended into 2021.
If a previously approved service is being provided after December 31, 2020, please call our Clinical Intake Department at the appropriate number and we will initiate a new authorization request or update the existing one. |
||
| Previously approved behavioral health testing (example: neuropsychological testing), IVF, DME |
To avoid duplication of cases and ineligibility issues due to changes in member coverage since the initial approval, prior authorizations will not be automatically extended into 2021.
If a previously approved service is being provided after December 31, 2020, please call our Clinical Intake Department at the appropriate number and we will initiate a new authorization request or update the existing one. For neuropsychological testing, new authorization requests will continue to have 365 days for the services to be completed. After that time, an authorization extension is required. |
||
| Vendor services (AIM) | Effective January 1, 2021, AIM will resume standard processes and authorize services for 60 days for commercial services; this does not apply to FEP. | ||
| Home health care Benefit limits still apply |
Medical necessity review required | HMO Notification only required PPO No notification required |
No notification required |
Clinical Intake Department Phone Numbers
| To request an authorization for |
Then |
|---|---|
|
Commercial members |
Call 1-800-327-6716 or fax 1-888-282-0780 |
|
Medicare HMO and PPO members |
Call 1-800-222-7620 or fax 1-800-447-2994 |
|
Federal Employee Program (FEP) |
Contact your local plan. In Massachusetts, call 1-800-689-7219 or fax |
|
Behavioral health |
Call 1-800-524-4010 or fax 1-888-641-5199 |
Medicare sequestration suspended through March 31, 2021
As part of the Consolidated Appropriations Act of 2021, Congress extended the suspension of the mandatory payment reductions known as “sequestration” through March 31, 2021. Beginning on April 1, 2021, sequestration will be reinstituted.
MPC_030620-1N-147-ART
This article is for providers who perform the services listed
We’re continuing to extend time-limited authorizations for outpatient procedures our members may not have been able to receive due to the COVID-19 emergency. All other administrative requirements related to these services continue to apply.
For the duration of the Massachusetts public state of emergency, we are granting extensions for the services listed below.
Assisted reproductive technology services
For assisted reproductive technology services listed in our medical policy that require prior authorization:
- We will extend existing authorizations for the period of January 1, 2020-June 30, 2020 to December 31, 2020.
- We will give new authorization requests 180 days for the service to be completed. After that time, an authorization extension would be required.
Neuropsychological testing services
For neuropsychological testing services listed in our medical policy that require prior authorization, we typically give the member 365 days to complete the authorized services. However, we’ve decided to extend existing authorizations for the period of March 1, 2019 – December 31, 2019 to December 31, 2020.
New authorization requests will continue to have 365 days for the service to be completed. After that time, an authorization extension would be required.
Added modifiers for non-emergency ground ambulance services
We have updated our previous April 20, 2020 article about our temporary coverage for non-emergency ground ambulance services to include the following modifiers:- NJ*: Skilled nursing facility to freestanding end-stage renal disease (ESRD) facility
- JN*: Freestanding end-stage renal disease (ESRD) facility to skilled nursing facility
*Note: Federal Employee Program member benefits may differ. Please visit fepblue.org.
Resources
April 20 news article (Non-emergency ground ambulance transports covered temporarily)
April 22 news article (COVID-19: Extending authorizations for specific services)
Questions
If you have questions, please contact our Clinical Coordination department at 1-800-327-6716.
MPC_030620-1N-108
This article is for medical providers who perform the services listed
We’re extending time-limited authorizations for outpatient procedures our members may not have been able to receive due to the COVID-19 emergency. All other administrative requirements related to these services continue to apply.
For the duration of the Massachusetts public state of emergency, we are granting extensions for the services listed below.
Assisted reproductive technology services
August 18, 2020 update: We've extended authorizations for these services. Read our August 18, 2020 news article to learn more.
For assisted reproductive technology services listed in our medical policy that require prior authorization:
- We will extend existing authorizations for the period of January 1, 2020-April 1, 2020 to September 30, 2020.
- We will give new authorization requests 180 days for the service to be completed. After that time, an authorization extension would be required.
Chiropractic services
For chiropractic services that require prior authorization through WholeHealth Networks, Inc. (WHN):
- We extended all finalized authorizations with a start date on or after February 1, 2020 by 120 days.
- As of March 31, 2020, the end dates have been extended 120 days for auto approved authorizations in the system.
- WHN’s clinical reviewers will manually adjust any authorizations that pend for clinical review and the clinical reviewer will extend the end dates by 120 days once the final determination is made.
Durable medical equipment
- We have extended existing authorizations through December 31, 2020.
High-technology radiology and obstructive sleep apnea testing and treatment
For the high-technology radiology and sleep testing and treatment services that require prior authorization with AIM Specialty Health:
- As of March 27, 2020, we have authorized new requests for 180 days to allow time to have the service performed.
Questions
If you have questions, please contact our Clinical Coordination department at 1-800-327-6716.
MPC_030620-1N-45
This article is for all providers caring for our members

As of January 1, 2023, CVS CaremarkTM will administer our prescription coverage as our pharmacy benefit manager. The company will do this for our commercial HMO/POS and PPO plan members, and for group Medex, Indemnity, and Medicare Advantage plan members.
This partnership will advance our commitment to quality and affordable health care for your patients, our members. We expect that it may lead to administrative simplification for our providers.
CVS Caremark is already the pharmacy benefit manager for our Federal Employee Program and Medicare Part D prescription drug plan members.
Express Scripts, Inc. (ESI) has been our pharmacy benefit manager for the last 20 years, and we’ve valued their partnership. ESI will continue to serve as administrator through the end of 2022.
We’ll share more information in the coming months.
Learn more
To learn more, read our press release.
MPC_080921-3R-1
This article is for dentists, oral surgeons, mental health providers, and primary care providers caring for our members
Intellectual disabilities may manifest any time before a child turns 18. They may affect intellectual functioning, such as learning, problem solving, judgement; and adaptive functioning, like the ability to perform activities of daily life.1 Developmental disabilities are a broader group of physical, intellectual, and/or behavioral conditions that begin during the developmental period and include conditions ranging from autism, Down syndrome, epilepsy, and cerebral palsy.2
Each patient with an intellectual and/or developmental disability has unique dental challenges due to their specific capabilities and abilities. Because dental health has been shown to impact overall health, dental and health care professionals can help their patients by encouraging them to get regular oral health care. Blue Cross is supporting your efforts by offering additional dental care benefits for members of Dental Blue with these conditions.
Dental care for patients with intellectual disabilities
Intellectual disabilities can vary in severity, but research shows that people with intellectual disability have more untreated caries (cavities) and a higher prevalence of gingivitis and other periodontal diseases than the general population, according to the National Institute of Dental and Craniofacial Research (NIDCR).3 Because people with intellectual disabilities may also have other conditions such as cerebral palsy, seizure or psychiatric disorders, attention deficit/hyperactivity disorder, or problems with vision, communication, and eating, NIDCR recommends taking a patient’s medical history before the dental visit. NIDCR’s fact sheet suggests many strategies for oral health care problems commonly found in patients with intellectual disabilities.
Dental care for patients with developmental disabilities
NIDCR also notes that people with developmental disabilities may each have distinct challenges in routine dental care, due to:
- Varied mental capabilities which may impact how well they can remember and execute daily care activities
- Behavior problems, including anxiety around receiving care in the dental office
- Mobility problems, which may affect their ability to manipulate a toothbrush or to access your dental office
- Neuromusculatural issues or uncontrolled body movements. 4
They note that patients with developmental disabilities may be more likely to have latex allergies, may be taking medications that dry their mouths, and may have damaging oral health habits such as teeth grinding and clenching. The Special Care Dentistry Association offers education and training for providers to learn more about the specific needs of patients with different developmental disabilities. 5
How Blue Cross is supporting our members
Because patients with intellectual and/or developmental disabilities can benefit from more frequent visits to a dental professional, we’ve expanded our Enhanced Dental Benefits. “At Blue Cross, we’re proud to be offering members with intellectual and developmental disabilities the opportunity for additional preventive dental care that will improve their oral health and their overall quality of life,” notes Robert Lewando, DDS, Executive Director of Dental Professional Services.
Members who have dental coverage with Blue Cross may receive additional cleaning, periodontal maintenance, oral cancer screening, and fluoride treatment benefits after their doctor or health care provider has signed an enrollment form to indicate their eligibility. These new benefits are available for members in new or renewing health plans on or after October 1, 2023.
What can providers do?
Both dentists and medical professionals have a role to play in helping their patients.
- Dental professionals can listen to their patients and their caregivers about the challenges they face in maintaining their dental care at home. Educate them about the additional benefits available to them by providing them with the member fact sheet and recommending that they work with the patient’s physician or clinician to enroll.
- Medical and mental health professionals can ask their patients whether they have dental health insurance with Blue Cross Blue Shield of Massachusetts and complete an Enhanced Dental Benefits enrollment form for those who are eligible.
1. psychiatry.org/patients-families/intellectual-disability/what-is-intellectual-disability
2.
cdc.gov/ncbddd/developmentaldisabilities/facts.html
3. nidcr.nih.gov/sites/default/files/2017-09/practical-oral-care-intellectual-care.pdf
4. nidcr.nih.gov/health-info/developmental-disabilities
5. scdaonline.org
MPC_010323-1P-11
This article is for:
- Primary care providers who refer patients for nutrition counseling
- Licensed dietician nutritionists
November 6, 2019 update:
We've updated this news article to clarify our referral requirements. Please see below for referral information.

We’re pleased to announce that we’re simplifying our coverage for nutrition counseling starting on January 1, 2020. We will no longer require an authorization for these services; however, services should still be medically necessary.
Note: Because of this change, we’ll remove the Medical Nutrition Therapy Authorization Extension form from Provider Central as of January 1, 2020.
Which members does this change apply to?
- Commercial HMO members
Is a referral for nutrition counseling still required?
- A PCP referral does not need to be entered; however, members should use an in-network provider for this service (for example, a licensed dietician nutritionist).
Questions?
For questions about this change, please contact your network representative at 1-800-316-BLUE (2583).
MPC_093019-1I-1-ART
This article is for hospitals, outpatient clinics, and other providers using gene therapies to treat our members
Before performing gene therapy services, such as CAR-T therapy, Kymriah, Luxturna, Yescarta, and Zolgensma, it’s important to know what’s covered.
Gene therapy involves altering the genes in a person’s body to treat or stop a disease.
The therapy may introduce new genetic material into a patient to replace or correct faulty or missing genetic material, or to make a new gene.
Does Blue Cross cover gene therapies?
Please be sure to check member benefits and eligibility before performing gene therapy services. Please note:
- Some self-insured employers do not offer their employees benefits for these therapies, so it’s important to check each member’s coverage.
- We're working to add a message to the 270/271 eligibility and benefit transaction. In the meantime, if you have questions, you can contact Provider Service.
- Because these are highly specialized therapies, most require prior authorization.
Review our medical policies
Our medical policies describe our coverage for gene therapy services, which may be through the member’s medical or pharmacy benefits. The medical policies contain prior authorization request forms that you can fill out and fax to us at the number listed on the form.
MPC_022720-2N-1
This article is for chloroquine and hydroxychloroquine prescribers
We are updating our standard Blue Cross formulary coverage for chloroquine and hydroxychloroquine (brand name: Plaquenil) for the duration of the COVID-19 public health emergency.
As of April 1, we have added a 10-day supply limit to these medications for:
- Members who are newly prescribed the medication for rheumatological and dermatological use (for example, to treat lupus, malaria, rheumatoid arthritis)
- Members using the medication for a COVID-19-related diagnosis.
If the member needs more than a 10-day supply (if they will be using it long-term for rheumatological and dermatological use, for example), you can request an authorization to cover more. To make this request, please submit the Massachusetts Standard Form for Medication Prior Authorization Requests (Click the link and find the form by choosing Authorization – Pharmacy). Or, contact our Clinical Pharmacy Operations area.
What about members who previously filled prescriptions for these medications?
Members who filled a prescription for rheumatological and dermatological use within the previous 180 days are excluded from the quantity limit. We’re contacting them to suggest that they take advantage of our early refill policy during this public health emergency, so they can have a supply of their medication. Some members may even contact you for a prescription for up to a 90-day supply from the Express Scripts Pharmacy®' (mail order).
Why is Blue Cross making this change?
You may be aware that on March 30, 2020, the Food and Drug Administration (FDA) issued an emergency authorization to use chloroquine and hydroxychloroquine as experimental coronavirus treatment.
The Massachusetts Division of Insurance (DOI) issued a March 26, 2020 Bulletin addressing this topic. The DOI asked insurers to continue covering these medications for rheumatologic or dermatologic conditions under their current policies. For COVID-19-related diagnoses, they asked insurers to add quantity limits.
What about members who have pharmacy coverage with another formulary?
For Federal Employee Program and Medicare Advantage members, coverage for these drugs remains the same at this time.
For members using the National Preferred Formulary (managed by Express Scripts, Inc.), there are new quantity limits for these medications.
Questions
If you have questions or need to request prior authorization, please contact Clinical Pharmacy Operations at 1-800-366-7778.
MPC_030620-1N-26
This article is for managers of intake, utilization review, and case management at acute care hospitals
Thank you for submitting your requests for NICU level of care authorizations for premature and medically complex infants to ProgenyHealth. Please use the chart below to determine when to submit a request to ProgenyHealth.
| If the baby is | Then |
|---|---|
| Discharged at the same time as the mother | No submission is required |
| Staying longer than the mother (Level 1) |
Submit inpatient notification to Blue Cross:
Submit surgical or outpatient services notification to Blue Cross:
|
|
Submit your request to ProgenyHealth:
|
To read more about this program, which we offer to our members at no additional cost, log in and go to News. Scroll down to the News Alert dated May 4, 2023: "Progeny will support premature and medically complex infants."
Resources
MPC_090722-2Q-14
On April 1, 2021, we reorganized some of the information on our Provider Central Clinical Resources page. We told you about these changes in our January 11, 2021 news article where we announced April 2021 Medical and Pharmacy Policy updates. We:
- Moved clinical criteria shown below to our Medical Policy site. You can search by the policy number or name to easily find them.
New policy # Policy name 142 Air ambulance* 146 Ground ambulance 158 Outpatient pediatric pain rehabilitation centers *Federal Employee Program guidelines for air ambulance will remain on the Coverage Criteria & Guidelines page in Provider Central.
- Transitioned the following guidelines to InterQual® Criteria. To access the criteria, you can log in and go to Clinical Resources>InterQual® Criteria & SmartSheets:
For Use this InterQual subset Crisis stabilization Residential crisis program Family stabilization Intensive outpatient (IOP)* Private duty nursing Private duty nursing *If you are looking for Intensive Community Based Treatment (ICBT), please see the ICBT subset.
- Retired our medical necessity criteria for:
- Outpatient Chest PT
- PT/OT Medical Necessity – Vestibular Rehabilitation
Please note that any information pertaining to the Federal Employee Program (FEP) is still available under Coverage Criteria & Guidelines.
MPC_012521-1E-1
This article is for primary care providers, gastroenterologists, and your clinical staff who suggest colorectal cancer screenings for patients
Shared decision making is a powerful tool when choosing the best treatment plan for your patients. When patients collaborate with their doctor, they’re more likely to advocate for themselves and learn more ways to treat and manage their condition.
In early October, we’ll start surveying members to find out whether they’ve talked to their health care provider about the various options for colorectal cancer screenings.
Results of these surveys will help:
- Inform future guidance around shared decision making.
- Improve the member experience when it comes to provider interactions.
- Improve quality measures around preventive care.
Here’s a link to our survey so you can see a sample of what we’ll ask our members.
Shared decision making is ethical, high-quality care

Mark Friedberg, MD, MPP
Senior Vice President, Performance Measurement & Improvement
Blue Cross Blue Shield of Massachusetts
"From an ethical standpoint, the best approach is to carefully explain to your patients the scientific evidence concerning all of the screening options available to them, to talk through the pros and cons of each screening option, to ask which screening option each patient wants, and to help each patient receive their chosen screening method,” says Mark Friedberg, MD, MPP, Blue Cross’ senior vice president, Performance Measurement & Improvement.
We believe the future of quality measurement should be grounded firmly in ethical principles that emphasize respect for persons and informed consent—which includes explaining all options for cancer screening.
Blue Cross conducted a pilot survey with members in March of 2023. The results suggested that the majority of our average-risk members who had a screening colonoscopy were never told about any other option. Adds Friedberg, "Studies of shared decision making strongly suggest that offering only colonoscopies lowers overall screening rates and worsens inequities in colorectal cancer screening rates.”
We anticipate reporting performance of shared decision making back to provider organizations as a starting point later this year.
US Preventive Services Task Force recommendations
When it comes to colorectal cancer screening, US Preventive Services Task Force recommends adults 45-75 should be screened for colorectal cancer. On their Colorectal Cancer Screening page, they list the various stool-based and direct visualization options and evidence.
We recommend reviewing the types of evidence for these screening modalities.
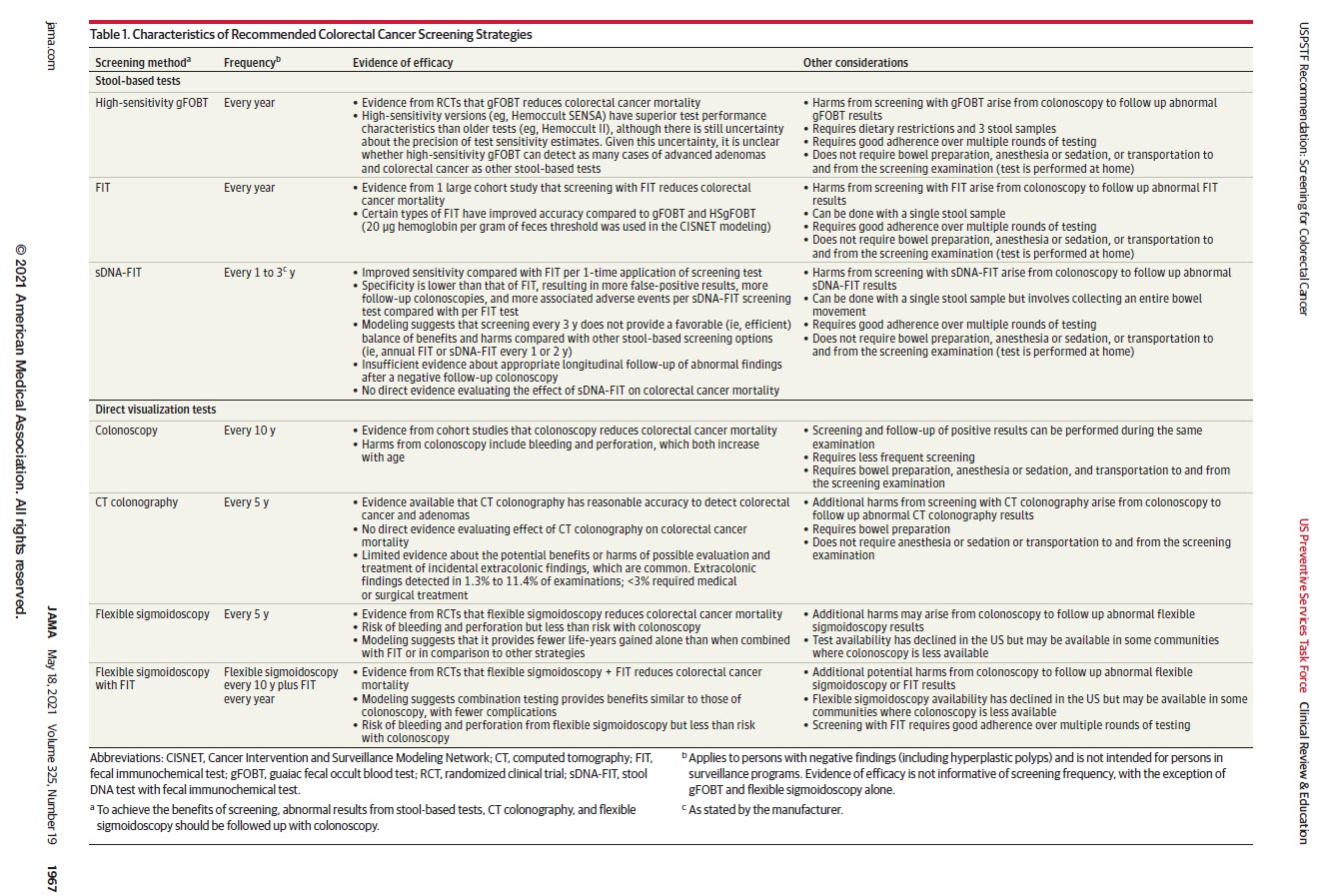
Source: JAMA. US Preventive Services Task Force. Recommendation Statement. Retrieved August 2023 at uspreventiveservicestaskforce.org.
Shared decision making in action
Some practices, such as Beth Israel Lahey Health Performance Network, have developed materials (translated into multiple languages) to help their patients understand their options and to give them a list of questions to ask their doctors as conversation starters.
Research shows that when providers explain all of a patient’s options and ask for and respect their values and preferences, patients are more likely to follow through with treatment and experience better health outcomes overall, according to Kim Ariyabuddhiphongs, associate chief medical officer at BILH's Performance Network.
Improving screening rates together
By surveying our members, we hope to help you improve your patients' experience and increase rates of colorectal cancer screening in an ethically sound manner.
Resources
US Preventive Services Task Force Colorectal Cancer: Screening
Doctor—and patient—know best
MPC_061223-1T-1
- Endocrinologists, pediatricians, and primary care providers who order continuous glucose monitoring devices for our members
- Durable medical equipment providers who supply the devices
In our monthly news article notifying you of upcoming medical policy changes, we listed an update to our Continuous Intermittent Monitoring of Glucose in Interstitial Fluid and Artificial Pancreas Device Systems medical policy 107. Now, we’d like to provide more details on the coverage changes we’re making that take effect on January 1, 2020.
CGM device coverage
We’re expanding coverage of continuous glucose monitoring (CGM) devices to commercial HMO/POS and Medicare HMO Blue members who have type II diabetes and meet the criteria listed in our policy.
CGM devices will require prior authorization for new starts or new devices
For our commercial HMO/POS and Medicare HMO Blue members with type I or type II diabetes, the codes for the CGM devices listed below will require prior authorization.
- Prior authorization is required only for new starts on the device or for existing members who need a new device. (Sensors and transmitters don’t require prior authorization).
- You can find the form to request prior authorization at the end of the medical policy.
| Codes that will require prior authorization | Devices |
|---|---|
|
Dexcom, Eversense, Libre, Medtronic |
Durable medical equipment providers
Please check to make sure there’s an authorization in place for the device to avoid rejected claims.
In addition, please remember that an approved authorization on file for the CGM device does not include coverage for the sensor (A9276) component of the device. The member still needs to have either pharmacy coverage, or a benefit rider attached to their medical coverage with Blue Cross, in order for any claim submitted for the sensor (A9276) component to process for payment.
MPC_100419-6F-1
This article is for prescribers caring for our members
Increasingly, members are taking advantage of home delivery of their maintenance medications through our latest collaboration with PillPack, an Amazon pharmacy. We’re promoting this option to members who are:
- Enrolled in a commercial, fully insured plan
- Taking two or more maintenance medications
- Not currently enrolled in our mail order program
What’s PillPack?
PillPack is a full-service retail pharmacy in the Express Scripts network. It offers:
- A 30-day supply of medication delivered every month
- Customized packaging with the date, time, medication name and strength, plus a medication label that has a picture of each pill and notes on how it should be taken
- Proactive contact with member’s doctor about prescription refills to ensure there are no gaps in medication
- Ongoing prescription checking to ensure there are no adverse medication interactions
- 24/7 access to pharmacists via phone, email, or online chat
What members pay
Members pay their regular retail pharmacy copayment or co-insurance. There are no additional subscription, service, or shipping fees.
Exclusive discounts
Members can save 25% on select vitamins and over-the-counter medications and include them in their shipment.
Easy sign up
Members can sign up easily through our secure MyBlue website or through our app. When they do this, they’ll have the added convenience of choosing to fill select maintenance medications based on their claims history.
Resources
View this video on the PillPack site for more information: https://www.pillpack.com/.
MPC_070120-1D-1
Update issued: April 18, 2023
We have clarified the definition of abortion
This article is for providers caring for our members
The Reproductive and Gender-affirming Care Act (Chapter 127 of the Acts of 2022) became effective January 1, 2023 as accounts renew, as we noted in our news article about 2023 changes to our products and benefits. The law:
- Mandates coverage for abortion and abortion-related care without cost share for fully-insured members for coverage upon renewal starting January 1, 2023.
- Accounts that are church or church-controlled organizations may opt out.
- Deductibles will apply to these services for high-deductible health plans, consistent with federal rules for HSAs.
- Provides legal protections around abortion, abortion-related, and gender-affirming care.
- Does not add new mandates related to gender-affirming care.
New guidance issued
The Division of Insurance recently issued Bulletin 2023-01 Relative to Abortion and Abortion-related Care. The Bulletin affirms the statutory definition of “abortion” as “any medical treatment intended to induce the termination of, or to terminate, a clinically diagnosable pregnancy except for the purpose of producing a live birth; provided, however, that ‘abortion’ shall not include providing care related to a miscarriage.” This definition includes surgical or medication-assisted (including Mifepristone in combination with Misoprostol or Misoprostal alone) abortions.
The Bulletin also affirms the application of an existing regulatory definition of “abortion-related care” to include the following services:
- Pre-operative evaluation and examination
- Pre-operative counseling
- Laboratory services, including pregnancy testing, blood type, and Rh factor
- Rh (D) immune globulin (human)
- Anesthesia (general or local)
- Post-operative care
- Follow-up
- Advice on contraception or referral to family planning services.
MPC_080222-1V-1-ART
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in December 2019 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in December 2020 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates, grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in December 2021 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in December 2022 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in December 2023 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
This article is for all providers caring for our members
We have decided to delay the implementation of our new Authorization Manager tool until 2021. We previously announced that this new self-service system would go live this November. (See News Alert dated July 9: A new way to submit and view authorization requests).
This delay will allow more time for provider training and a more effective transition to the new system. Authorization Manager provides a new way to submit authorization requests and check on the status of submitted authorizations for all of our members. It builds on the system we launched in February specifically for providers caring for our Medicare Advantage members.
We will notify you of the new implementation date and detail the changes you will experience with authorization processes when they become available.
Questions?
If you have any questions, please call Network Management and Credentialing Services at 1-800-316-BLUE (2583). As always, thank you for the care you provide to your patients—our members.
MPC_012618-1L-29
While opioid misuse is an ongoing safety and health care quality issue for our community, local efforts to fight this epidemic are making a difference. According to the Massachusetts Department of Public Health, the rate of opioid-related overdose deaths in 2019 is an estimated 6% lower compared to 2016.
 Dental Blue providers contributed to this effort by prescribing fewer opioid prescriptions while continuing to treat their patients safely and effectively. We’ve seen a decrease in opioid prescriptions written for our members each quarter since the start of 2018. In the first quarter of 2018, Dental Blue dentists wrote 1,226 prescriptions for opioids for our members, compared to 809 in the first quarter of 2020, a 34% decrease.
Dental Blue providers contributed to this effort by prescribing fewer opioid prescriptions while continuing to treat their patients safely and effectively. We’ve seen a decrease in opioid prescriptions written for our members each quarter since the start of 2018. In the first quarter of 2018, Dental Blue dentists wrote 1,226 prescriptions for opioids for our members, compared to 809 in the first quarter of 2020, a 34% decrease.
This significant decrease is due to dentists:
- Prescribing short-acting opioids for acute pain very responsibly.
- Prescribing small amounts of pain medication and following up with patients before writing additional prescriptions. The total days' supply fell from 4,242 pills in the first quarter of 2018 to approximately 2,714 pills in the first quarter of 2020, a 36% drop.
- Looking at non-opioid alternatives for patient pain management.
Thank you, Dental Blue providers, for being key to improving our short-acting opioid treatment protocols.
Here’s how we continue to work together to fight opioid use in Massachusetts:
- Massachusetts dental and medical schools continue to teach courses in how to manage pain, prescribe painkillers, and detect abuse of those drugs.
- The Massachusetts Dental Society, working with local dental schools and the Commonwealth, mandates continuing education courses in pain management and substance use. All practicing dentists must be refreshed in them at every licensure renewal.
- Our policies for physician and dentist opioid prescriptions limit the days' supply of opioids to minimize the likelihood of addiction. Providers are required to check the state registry before writing a prescription to make sure patients do not have other current opioid prescriptions.
MPC_031120-1L-12
This time last year, no one ever heard of the COVID-19 virus. Even six months ago, few had any inkling as to what it would do to the dental profession. Since then, dental offices have been closed in Massachusetts except for emergency care, making these difficult times for the dental profession.
In phase one of the Commonwealth’s reopening plan, dentists have been allowed to treat patients who have emergent dental needs. Emergent care is for patients who may not have pain or swelling due to trauma or a dental infection but who, without some intervention, would need emergency treatment shortly. When treating these patients, you may use CDT code D1354, interim caries medicament application, if it is applicable to the emergent situation.
Billing for emergent care needs
Consider using CDT D1354 to bill for the application of a medicament to treat patients for advanced caries on a tooth where you may be otherwise unable to perform definitive care. For example, it could be used when you want to avoid treatment with a handpiece to minimize aerosol or for treatment plans that minimize patient appointment duration. Although this limited treatment doesn’t substitute for definitive care, it could provide your patient with interim care while helping to keep you, your office staff, and your patients safe.
| CDT code | Narrative |
|---|---|
| D0140 | Limited oral evaluation—problem-focused. This code is suggested for reporting telephonic or virtual visits* |
| D1354 | Interim caries-arresting medicament application per tooth* |
*subject to benefit coverage and CDT guidelines
Reminder about personal protective equipment
In a News Alert that we published on May 28, we noted that personal protective equipment (PPE) is considered a component of infection control and is not separately billable to the member. Our News Alert stated that billing for PPE with D1999 will cause claim denials. Only code D1999 will be denied; we will process all other covered services itemized on your claim.
If you bill for D1999, both you and the member will receive a reject message noting that the member should not be billed for PPE. Additionally, you may not collect pre- or post-service payment from the member for this expense.
Thank you!
We will continue to partner with the dental community as offices begin to reopen. We thank your whole dental team for their dedication to your profession and to your patients, our members.
MPC_030620-1N-56
Dentists who care for our pediatric members.
The Centers for Disease Control and Prevention and the Massachusetts Department of Public Health have both reported alarming drops in vaccination rates over the last few months. Some parents have concerns about bringing their children into the medical office during the COVID-19 pandemic, but the importance of keeping vaccines current is critical.
We are asking you to please encourage your dental patients to keep their vaccinations up-to-date.
Dr. Robert Lewando, DDS, Director of Dental Operations, notes that "Dentists play an important role in maintaining their patients’ overall health. Just as dentists have helped encourage parents to get the HPV vaccine for their children, directing the parents to consult their child’s medical office about staying current on all of their vaccinations can significantly help our members."
Please see the resources below that you may share with your patients.
How we're reminding members to stay on their vaccination schedule
We want you to know that we’re encouraging our members—your patients—to reach out to their medical provider if they aren’t current with their vaccines. In late July, we’re sending emails and texts to the parents or guardians of the following members, with these recommendations:
| Age group | Should receive |
|---|---|
| Children |
All should be received by the second birthday. |
| Adolescents |
|
| Sample email messages | |
| Childhood | Adolescent |
 |
 |
We also send these emails in Spanish.
As always, thank you for the care you give your patients, our members.
Resources
![]() HPV fact sheet for members (English)
HPV fact sheet for members (English)
![]() HPV fact sheet for members (Spanish)
HPV fact sheet for members (Spanish)
![]() HPV vaccination tips (webinar slides)
HPV vaccination tips (webinar slides)
CDC vaccines & immunizations
Why it's important for kids to get vaccinated now (Coverage article for members)
For FEP specific information, visit
fepblue.org
MPC_072020-1H-1
This article is intended for pediatricians, family practitioners, dentists, and their office staff
On September 12, we hosted a live webinar about the HPV vaccine and offered tips to help improve vaccination rates. During the webinar we discussed:
- How the HPV vaccine can prevent HPV cancers from developing
- The importance of your recommendation to parents
- How dentists can help support HPV vaccination adoption
- Tips for how to talk to your patients about the vaccine
Thank you to everyone that was able to attend and join our discussion. If you were unable to attend, please see our recorded webinar.
We are sending a brief feedback survey to all who registered. Please take the time to answer these questions which will help us improve future sessions.
Resources
![]() HPV fact sheet for members
HPV fact sheet for members![]() HPV Vaccination Tips webinar slide deck
HPV Vaccination Tips webinar slide deck
As always, thank you for the care you provide to your patients—our members.
MPC_051619-1B-8
This article is for prescribers of infused and injected medications
As we announced in an October 1, 2021 News Alert, we decided to make our Site of Care program for infused and injected medications voluntary rather than a requirement. Below, we describe what this means for medications you may prescribe and what we’re telling our members.
The Site of Care program is designed to promote the use of infused and injected medications in the most cost-effective, clinically appropriate setting. Making this program voluntary gives members options on where we’ll cover their medication.
You can continue to follow your current process for these medications for our commercial (HMO, POS, and PPO) and indemnity members. This includes:
- Requesting authorization for the medications listed below with an asterisk, just as you do currently. Please refer to the medication’s medical policy for medical necessity criteria we use to make a coverage determination.
- Note: If you recently received authorization for a drug listed below (noted with an asterisk) with an end date of December 31, 2021, we’ve extended the authorization for one year from the original approval date.
- Assessing patients who may wish to receive their medication in an alternate site of service, such as home infusion therapy. We hope you’ll join us in discussing the benefits of home infusion therapy with your patients when it’s a clinically appropriate option for them.
Here’s a list of home infusion therapy providers in Massachusetts that have access to these medications.
For patients taking Enytvio or Ocrevus, you can refer to any in-network home infusion therapy provider. We’re also working closely with New England Life Care, and they are prepared to take new referrals.
| Infused or injected medications | |||||
|---|---|---|---|---|---|
| Aldurazyme | Crysvita | Givlaari* | Lemtrada* | Ruconest* | VPRIV* |
| Aralast* | Duopa | Glassia* | Lumizyme | Soliris* | Vyepti* |
| Benlysta | Elaprase | Haegarda* | Naglazyme | Tysabri* | Vyondys 53* |
| Berinert* | Elelyso* | Ilumya* | Ocrevus | Ultomiris* | Xolair* |
| Cerezyme* | Entyvio* | Kalbitor* | Onpattro* | Uplizna* | Zemaira* |
| Cinqair* | Exondys 51* | Kanuma* | Prolastin* | Viltepso* | |
| Cinryze* | Fabrazyme | Krystexxa | Radicava | Vimizim | |
*This medication requires prior authorization. Refer to Medical Utilization Management (MED UM) & Pharmacy Prior Authorization Policy 033.
We’re advising patients taking the drugs noted above that they continue to have options on where they receive their medication, and that home infusion therapy is a covered option.
Members who received previous letters from us about our Site of Care policy will receive information encouraging them to speak with their doctors to determine if home infusion therapy is a good option for them.
![]() Member fact sheet
Member fact sheet ![]() Member fact sheet for Entyvio and Ocrevus. Members can use any in-network home infusion therapy provider for Entyvio and/or Ocrevus. We’re also working closely with New England Life Care, and they are prepared to take new referrals.
Member fact sheet for Entyvio and Ocrevus. Members can use any in-network home infusion therapy provider for Entyvio and/or Ocrevus. We’re also working closely with New England Life Care, and they are prepared to take new referrals.
|
|
Convenience. Home infusion therapy allows your patients to receive treatment in the comfort of their own home from experienced nurses and pharmacists. Specialized pharmacists provide compounded medications or nutrition for individual patients according to their personalized care plan developed with the patient, their caregivers, and their physician or medical team. Medications are delivered to your patient’s home where specialized nurses teach them how to manage their nutritional and biologic treatments while solely focused on monitoring their advanced home care. If they have questions, help is available 24/7 from their home infusion therapy provider. |
|
|
Costs. Home infusion therapy is often less costly than other sites of care, so your patient could save money by switching. |
|
|
Time. Your patients can save time spent commuting to their treatment. Many patients appreciate being able to receive their infusion at home where they spend time working or relaxing. |
If you have any questions, please call Clinical Pharmacy Operations at 1-800-366-7778.
- Home infusion therapy providers: Infused and injected medications
- Home infusion therapy page
- Home infusion therapy member fact sheet
- Member fact sheet for Entyvio and Ocrevus
- October 1, 2021 News Alert: Update to Site of Care for infused, injected medications
To access this News Alert, log in and click News. Look for the October 1, 2021 date and scroll to the News Alert called, “Update to Site of Care for infused, injected medications.”
MPC_032221-1M-25
By: Rachel Coppola for Coverage, a news service of Blue Cross Blue Shield of Massachusetts
Agrowing movement toward engaging patients in their own health care and treatment decisions is gaining momentum among clinicians and health plans, and improving health outcomes while helping to address health inequities.
For example, at Beth Israel Lahey Health, a new effort encourages patients to play a greater role in deciding the type of colorectal cancer screening they will get.
The work has led to a 10% increase in overall colorectal cancer screening rates, including a 15% increase in less-invasive at-home tests.

“The results we are seeing are very exciting,” said Dr. Kim Ariyabuddhiphongs, associate chief medical officer at BILH's Performance Network, who is leading this work. “At BILH, we strive to help our patients and their families live healthier lives and believe strongly in the importance of patient engagement. We began this effort two years ago with a group of 200 physicians who care for hundreds of patients as a way to both improve the patient experience and increase colorectal cancer screening rates.”
Currently, BILH is expanding this effort to reach more of its patients, Ariyabuddhiphongs said. “Every month a new cohort of patients becomes eligible for outreach.”
Research shows that when providers explain all of a patient’s options and ask for and respect their values and preferences, patients are more likely to follow through with treatment and experience better health outcomes overall, she noted.
Starting a conversation
As part of the program, patients approaching age 45 or who have health factors that put them at a greater risk for developing colorectal cancer receive an email before their upcoming doctor appointment referring them to a decision aid that was designed with input from patients and clinicians and has been translated into six languages.

For instance, a colonoscopy involves more prep and procedure time and is a more invasive procedure, but can be performed just once every several years for most patients. A home screening test is more convenient and less invasive, but must be completed every year.
“Our team identified colorectal cancer screening as a good fit for greater patient engagement because there are multiple options patients can choose that have different impacts on their daily life,” Ariyabuddhiphongs said. “We decided to send the decision aid in advance of the doctor visit because we want patients to learn about their options so they can have an informed discussion with their provider and then come to a shared decision about which tests to undergo, if any.”
Shared decision-making is a shared goal
The concept of “shared decision-making” between patients and providers is a shared goal among many health care providers and health plans, including Blue Cross Blue Shield of Massachusetts.
“We want to encourage all providers to make shared decisions with their patients on important health care matters,” said Dr. Mark Friedberg, an internist and senior vice president of performance measurement and improvement at Blue Cross.
When it comes to their care, we believe patients should understand the options they have, talk through those with their clinician, and come to a shared decision that is consistent with their values and preferences

Dr. Mark Friedberg said
In addition to improving the patient experience and the quality of care patients receive, Friedberg says the approach also helps reduce racial inequities in care, a priority for the health plan.
Data from the health plan reflecting claims for 1.3 million Blue Cross members reveals that colorectal cancer screening rates are 7% lower among Hispanic patients than white patients and 10% lower among Black patients.
Ariyabuddhiphongs noted that her team is analyzing the data from this effort to see if it decreased racial and ethnic inequities in colorectal screening rates among patients.
Soon, Blue Cross would like to integrate shared decision-making measures into the quality measures it uses to pay providers, just as it aims to integrate health equity measures into provider contracts. That would provide financial rewards to practices that adopt shared decision-making practices, just as the insurer has long provided financial incentives for high-quality, high-value care.
Charting progress
Ariyabuddhiphongs said BILH conducted provider and patient surveys before launching the decision aid and will continue to conduct surveys to chart the initiative’s progress. They also will continue to monitor colorectal cancer screening rates.
Initial feedback from clinicians has been positive, Ariyabuddhiphongs said.
“Providers have told us they like having the decision aid to prompt and facilitate a discussion around screening. They tell us, ‘Patients will bring this issue up before I do.’ ”
She said BILH is exploring other areas to expand the program, including screening for breast, lung and prostate cancer, advanced care planning, and treatment for patients with diabetes.
We want to do all we can to ensure patients have the information and support they need to discuss their care with their clinician and make decisions that are going to be the best for them and their families
Ariyabuddhiphongs said.
Coverage is a news service of Blue Cross Blue Shield of Massachusetts.
This article is for health care providers who bill for flu vaccinations.
Cold and flu season is here, and we need your help protecting our members – your patients. As you know, your patients can protect themselves and everyone around them by receiving the flu vaccine.
Here is some important information about Blue Cross coverage and billing information for the flu vaccine, and several reminders of its importance.
What Blue Cross covers
Blue Cross follows the CDC and Advisory Committee on Immunization Practices recommendations for the 2023-2024 season.
- In-network. We cover the cost of all CDC-approved vaccines, based on availability, when administered by an in-network provider.
- Out-of-network. We cover flu vaccines performed by non-participating providers only for Medicare Advantage members.
Billing information
- Bill only the applicable CPT or HCPCS codes listed on your fee schedule.
- We provide separate reimbursement for both the COVID-19 vaccine and flu vaccine (see below for the administration), even if a member receives both during the same office visit.
- We provide separate reimbursement for the administration (injection) of routine pediatric immunizations (0-19 years) even if it is part of an office visit.
- For members ages 20 and older, we do not separately reimburse for the administration (injection) of immunizations when billed with an office visit.
- See our Flu Season fact sheet for more information.
Protecting each other
Remind your patients that the flu vaccine protect not just themselves, but everyone around them and especially those who have the highest risk.
As you know, getting a flu shot reduces the risk of:
- Getting the flu or having a severe case of it
- Spreading the flu to family, friends, and community
- Being hospitalized
- Contracting COVID-19 and the flu (two life-threatening diseases) simultaneously
The risk of COVID-19 remains
While the COVID-19 public health emergency expired earlier this year, COVID-19 remains a risk to patients. The CDC recommends an updated COVID-19 vaccine or booster to protect against potentially serious outcomes, including Long COVID.
CDC recommendations for 2023-2024
- The Centers for Disease Control and Prevention (CDC) recommends everyone over the age of six months receive routine flu vaccinations, unless there are contraindications, such as a history of severe, life-threatening allergies to the flu vaccine.
- While vaccination should ideally occur by the end of October, it can occur as long as influenza viruses are circulating.
High-risk groups include:
- Adults 65 years and older
- Children younger than two years old
- People with weakened immune systems due to disease or medications
- Those who are pregnant or are up to two weeks postpartum
- People who live in nursing homes and long-term care facilities
Resources
- See our Flu Season fact sheet (link to fact sheet) and Immunizations Payment Policy (log in required) for more details about vaccines and how to bill for vaccine administration.
- Visit the CDC website flu page.
- For information on where to get a flu shot, your patients can visit our Find a Doctor & Estimate Costs tool (bluecrossma.com/findadoctor), bcbs.com, or vaccines.gov/get-vaccinated/where.
MPC_101623-2S-1
This article is for health care providers who bill for flu vaccinations.
Cold and flu season is here, and we need your help protecting our members – your patients. With flu season peaking between December and February, now is the time to encourage your patients to take the annual flu vaccine, which is free of charge for most Blue Cross Blue Shield of Massachusetts members.
Here, we’ll share important information about Blue Cross coverage and billing information for the flu vaccine, as well as several reminders on its importance.
What Blue Cross covers
Blue Cross follows the Centers for Disease Control and Prevention (CDC) and Advisory Committee on Immunization Practices recommendations for the 2022-2023 season.
- In-network. We cover the cost of all CDC-approved vaccines, based on availability, when administered by an in-network provider.
- Out-of-network. Only Medicare Advantage members will be reimbursed for flu vaccines performed by non-participating providers.
Billing information
- Bill only the applicable CPT or HCPCS codes listed on your fee schedule.
- We provide separate reimbursement for both the COVID-19 vaccine and flu vaccine (see below for the administration), even if a member receives both during the same office visit.
- We provide separate reimbursement for the administration (injection) of routine pediatric immunizations (0-19 years) even if it is part of an office visit.
- For members ages 20 and older, we do not separately reimburse for the administration (injection) of immunizations when billed with an office visit.
- We do not reimburse for vaccines that are available for free from the state.
Early CDC data on outpatient visits for flu-like illness
Data from the CDC show that patients are making significantly more visits to their doctors’ offices in the early part of the 2022-2023 flu season than in any of the past five flu seasons. As we slowly move away from precautions that became commonplace in the early years of the COVID-19 pandemic, flu-like illnesses could be seen at higher rates than we’ve seen in recent years.
Source: https://www.cdc.gov/flu/weekly/index.htm
Protecting each other
Promote the flu vaccine to your patients with a reminder that it helps to reduce the spread of the virus to their loved ones. This is especially true with high-risk populations, such as people with certain chronic conditions and adults over 65.
As you know, getting a flu shot reduces the risk of:
- Getting the flu or having a severe case of it
- Spreading the flu to family, friends, and community
- Hospitalization
- Contracting COVID-19 and the flu (two life-threatening diseases) simultaneously
If we each do our part and get vaccinated, we can lessen the effects of this year’s flu season just like we did last year.
The continued impact of COVID-19
While diminished, the COVID-19 pandemic continues to affect thousands of patients and to strain health care capacity. This makes it especially important for patients to receive the flu vaccine this.
Fortunately, the flu vaccine and COVID-19 booster shot can be administered during the same visit and co-administered within 14 days.
CDC recommendations for 2022-2023
- The CDC recommends everyone over the age of six months receive routine flu vaccinations, unless there are contraindications, such as a history of severe, life-threatening allergies to the flu vaccine.
- Vaccination should continue throughout the season as long as influenza viruses are circulating.
High-risk groups
- Adults 65 years and older
- Children younger than two years old
- People with weakened immune systems due to disease or medications
- Those who are pregnant or are up to two weeks postpartum
- People who live in nursing homes and long-term care facilities
Resources
- See our Flu Season fact sheet and Immunizations Payment Policy for more details about vaccines and how to bill for vaccine administration.
- Visit the CDC website flu page.
- For information on where to get a flu shot, your patients can visit our Find a Doctor & Estimate Costs tool (bluecrossma.com/findadoctor), bcbs.com, or vaccines.gov/get-vaccinated/where.
Resources
- See our Flu Season fact sheet and Immunizations Payment Policy for more details about vaccines and how to bill for vaccine administration. (To download the payment policy, log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.)
- Visit the CDC website flu page.
- For information on where to get a flu shot, your patients can visit our Find a Doctor & Estimate Costs tool (bluecrossma.com/findadoctor), bcbs.com, or vaccines.gov/get-vaccinated/where.
- Coverage article: Perfect timing for flu and COVID shots.
MPC_102822-2F-1
This article is for orthopedic surgeons, rehabilitation facilities, and rheumatology providers who administer epidural steroid injections
We cover epidural steroid injections for neck and back pain as outlined in our existing medical policy 690: Epidural Steroid Injections for Neck and Back Pain.
Epidural steroid injections performed with fluoroscopic guidance may be considered medically necessary for the treatment of neck and back pain when the following criteria are met:
- Lumbar or cervical radiculopathy (sciatica) that is not responsive to at least four weeks of conservative management
- Persistent pain is present of at least moderate-severe intensity
- Short-term relief of pain is the anticipated outcome
Conservative nonsurgical therapy for at least four weeks should include the following:
- Use of prescription strength analgesics, which include anti-inflammatory medications with or without adjunctive medications such as nerve stabilizers or muscle relaxants, at a dose sufficient to induce a therapeutic response
- Participation in at least four weeks of physical therapy (including active exercise) or documentation of why the patient could not tolerate physical therapy
- Evaluation and appropriate management of associated cognitive and behavioral issues
Repeat treatment of persistent pain due to radiculopathy (sciatica) may be considered medically necessary under the following conditions:
- Previous epidural steroid injections were successful at relieving pain
- At least 30 days have passed since the last injection
- No more than six injections are given over a 12-month period.
Payment policy application
- Enforcement of this medical policy occurs through system edits and post-payment reviews.
- We continually expand our ability to process claims in accordance with this policy pre-payment, which will reduce the number of claims we review post-payment.
Resources
The codes and diagnoses listed in medical policy 690: Epidural Steroid Injections for Neck and Back pain, will be updated on our website in January 2022. To download this medical policy, please visit our medical policy site.
On January 24, 2022 the Food and Drug Administration (FDA) revoked emergency use authorization (EUA) for two monoclonal antibody treatments—bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) because they are not effective against circulating COVID variants. As a result, these treatments are no longer covered by Blue Cross until further notice from the FDA.
According to the FDA statement: “Because data show these treatments are highly unlikely to be active against the omicron variant, which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.”
You may now enroll Federal Employee Program (FEP) members into our home-based advanced illness care pilot program. This program aims to improve care for our members who have an advanced disease, disorder, or condition. We urge you to consider referring any Blue Cross of Massachusetts members – except those in Medicare Advantage, Indemnity, HMO Blue Essential, and Harvard and MIT plans.
Benefits of referring your patients
Similar programs studied have shown that home-based care for patients with advanced illness:
- Increases quality of life and satisfaction with care for patients and their families
- Allows members to be cared for at home, where appropriate, instead of in an inpatient or hospital emergency department.
Please review our Referring Provider fact sheet for more information about member eligibility and referrals.
Enrolled members will benefit from:
- In-home visits from an interdisciplinary care team including physicians, nurses, social workers, and spiritual care providers
- 24/7 access to home urgent care visits
- Telephone access for symptom advice and concerns
- Caregiver support and respite
- Case management
- Advanced care planning.
The participating agencies will coordinate care with you and keep you informed about changes in your patient’s status.
Cost
- For commercial members, copays, co-insurance, and deductible rates apply to this program pilot and will be billed as a single specialty medical care visit for each month of services.
- For Federal Employee Program members, there is no cost.
Service area
We’ve partnered with agencies serving most areas of the state to provide these services to our members. There is currently no coverage in Franklin and Berkshire Counties, Cape Cod and the Islands, or the towns of Athol, Chesterfield, Goshen, Plainfield, Royalston, and Williamsburg.
MPC_041118-2P-12
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in February 2020 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in February 2021 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in February 2022 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in February 2023 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in February 2024 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
This article is for health care providers who bill for flu vaccination.
Flu season has begun, and we’d like to remind you of our coverage and reimbursement for flu vaccinations.
CDC recommendations
- The Centers for Disease Control and Prevention (CDC) recommends routine flu vaccination for everyone over the age of six months unless there are contraindications, such as a history of severe allergic reaction to the vaccine.
- Ideally, vaccination should take place by the end of October.
What Blue Cross covers
Blue Cross follows the CDC and Advisory Committee on Immunization Practices (ACIP) recommendations for the 2019-2020 season.
Services are covered without a cost to our members.
Please be sure to bill only codes listed on your fee schedule. You can check your fee schedule for covered codes.
How to learn more about the flu
- See our flu season fact sheet more details about vaccines and how to bill for vaccine administration.
- For more flu-related information, visit bluecrossma.com/flu.
MPC_091119-1W-1-ART
This article is for health care providers who bill for flu vaccinations.
Getting an annual flu shot is always important, but this year it’s particularly critical as we continue to deal with the COVID-19 pandemic. Please encourage your patients to get the vaccine. Most Blue Cross members will pay nothing when vaccinated.
Why it’s important
Widespread flu vaccination will help lessen the strain on our healthcare system during the current pandemic.
Also, patients who get a flu shot will reduce their risk of:
- Getting the flu (or having a severe case if they do get it)
- Spreading the flu to their family, friends, and community
- Hospitalization
- Contracting COVID-19 and the flu (two life-threatening diseases) simultaneously
CDC recommendations for 2020-2021
- The Centers for Disease Control and Prevention (CDC) recommends everyone over the age of six months receive routine flu vaccinations, unless there are contraindications such as a history of severe, life-threatening allergies to the flu vaccine.
- Ideally, vaccination should take place in September or October.
High risk groups
- Adults 65 years and older
- Children younger than two years old
- Pregnant women and women up to two weeks after the end of pregnancy
- American Indians and Alaska Natives
- People who live in nursing homes and long-term care facilities
What Blue Cross covers
Blue Cross follows the CDC and Advisory Committee on Immunization Practices recommendations for the 2020-2021 season.
- In-network. We cover the cost of all CDC-approved vaccines, based on availability, when administered by an in-network provider.
- Out-of-network. Only Medicare Advantage members will be reimbursed for flu vaccines performed by non-participating providers.
How to bill
Bill only codes listed on your fee schedule.
Resources
- See our Flu Season fact sheet and Immunizations Payment Policy (log in required) for more details about vaccines and how to bill for vaccine administration.
- Visit the CDC website flu page.
- For information on where to get a flu shot, your patients can visit our Find a Doctor & Estimate Costs tool (member.bluecrossma.com/fad), bcbs.com, or vaccines.gov/get-vaccinated/where.
MPC_071320-1R-1
This article is for health care providers who bill for flu vaccinations.
Last year saw a decline in flu-related hospitalizations and deaths, most likely attributed to the COVID-19 vaccine and related measures, such as face masks and social distancing. As restrictions ease across the country, it becomes increasingly critical to get an annual flu shot now more than ever before. Please encourage your patients to get the vaccine. Most Blue Cross members will pay nothing when getting vaccinated.

"It’s easy to lose track in the current COVID pandemic, but there are tens of thousands of seasonal flu deaths each season,” says Dr. Daniel Kuritzkes, chief of infectious disease at Brigham and Women’s hospital. “A lot of that is preventable with the vaccine." Read more of his thoughts in our Coverage story, here. |
What Blue Cross covers
Blue Cross follows the Centers for Disease Control and Prevention (CDC) and Advisory Committee on Immunization Practices recommendations for the 2021-2022 season.
- In-network. We cover the cost of all CDC-approved vaccines, based on availability, when administered by an in-network provider.
- Out-of-network. Only Medicare Advantage members will be reimbursed for flu vaccines performed by non-participating providers.
Billing information
- Bill only the applicable CPT or HCPCS codes listed on your fee schedule.
- We provide separate reimbursement for both the COVID-19 vaccine and flu vaccine (see below for the administration), even if a member receives both during the same office visit.
- We provide separate reimbursement for the administration (injection) of routine pediatric immunizations (0-19 years) even if it is part of an office visit.
- For members ages 20 and older, we do not separately reimburse for the administration (injection) of immunizations when billed with an office visit.
- We do not reimburse for vaccines that are available for free from the state.
- See our Flu Season fact sheet for more information.
Avoiding a “Twindemic”
The extended length of the COVID-19 pandemic has resulted in more public interaction as states and venues open up. As more individuals deal with precaution fatigue, the greater the likelihood of an increased number of flu illnesses.
As hospitals nationwide continue to be at or over capacity, a surge of flu patients on top of an ongoing pandemic would be severely overwhelming. Widespread flu vaccination will help lessen the strain on our health care system.
Protecting each other
You can promote the vaccine to your patients with a reminder that it helps to reduce the spread of the virus to their loved ones. This is especially true with high-risk populations, such as those who are pregnant or have certain chronic conditions, adults over 65, and kids under 12 who aren’t currently eligible to receive their COVID-19 vaccine.
If we each do our part and get vaccinated, we can lessen the effects of this year’s flu season just like we did last year.
Resources
- See our Flu Season fact sheet and Immunizations Payment Policy (log in required) for more details about vaccines and how to bill for vaccine administration.
- Visit the CDC website flu page.
- Visit the mass.gov flu prevention and vaccine information page.
- For information on where to get a flu shot, your patients can visit our Find a Doctor & Estimate Costs tool (bluecrossma.com/findadoctor), bcbs.com, or vaccines.gov/get-vaccinated/where.
MPC_083021-1T-1
This article is for prescribers caring for our members
We’re planning to make changes to our standard Blue Cross formulary in the fourth quarter of 2020 that include:
- Moving medications to non-covered
- Excluding medications from coverage
- Making tier changes
- Adding quality care dosing limits
- Adding step therapy to certain medications
- Updating pharmacy medical policies
We’ll provide you with more details later this summer.
MPC_121119-1S-14
This article is for:
- Genetic counselors
- Providers who order genetic tests
- Laboratories that perform genetic tests
Since implementing a prior authorization program with AIM Specialty Health®′, we have noticed situations in which the authorized test or tests do not match the services billed by the laboratory performing the test.
We would like to share the following best practices with providers ordering genetic tests and those performing them. Following these best practices will help with claims processing and members avoiding costs for non-authorized services.
Please remember to request prior authorization from AIM before you send the specimen to the lab. As part of your contract with us, you’re required to follow our medical management policies.
Here are additional best practices:
- Once you’ve submitted your authorization request, you’ll receive a response. If your authorization is approved, AIM ProviderPortalSM will indicate it’s “Authorized” in the Order Request Preview (see (see
 in the example below).
in the example below).

- Tell the member that they must have the test within the timeframe approved (see
 in example). Otherwise, if the test is outside of those dates, a new authorization request will be needed.
in example). Otherwise, if the test is outside of those dates, a new authorization request will be needed. - Attach a copy of the approved authorization to your lab requisition form. This will help the lab understand what's been approved. You’ll be able to download a PDF or print a copy (see
 in example) after you have submitted your authorization request and it’s been approved.
in example) after you have submitted your authorization request and it’s been approved.
- Click "View Details" (
 in example) to see all CPT codes associated with the test that are approved. Remember: You will need to make sure you have approval for each CPT code.
in example) to see all CPT codes associated with the test that are approved. Remember: You will need to make sure you have approval for each CPT code.
- Click "View Details" (
Important: We recommend attaching a copy of the approved authorization to your lab requisition instead of using a pre-populated lab requisition form, such as the one in the example below. When you enter the test into AIM’s ProviderPortal, you are requesting the individual test, not a panel, so the test authorized and the pre-populated form are not always a match.

When a specimen comes into your lab for genetic testing, before you analyze the specimen, please remember to verify:
- An approved authorization for the test. You can verify the authorization approval by going to the AIM ProviderPortal.
- The CPT codes approved as part of that authorization. Next, you can give those codes to your billing department for your claim, so your claims will process smoothly.
- Click "View Details" (See in the example) to see any CPT codes associated with the test that are approved.
- Click "View Details" (See
Additional information about the program
- Provider Central's Genetic Testing page (now available without logging in)
- AIM resources
- AIM Step-by-step tutorials
Questions?
For questions about the genetic testing prior authorization program with AIM, call Network Management and Credentialing Services at 1-800-316-BLUE (2583).
MPC_112217-1T-20-ART
This article is for all providers requesting inpatient surgery authorization
As of September 1, 2021, Authorization Manager will allow you to request authorizations for certain procedures performed in an inpatient setting, including emergency surgery. The InterQual® SmartSheet information you used to submit to us separately is now integrated into the tool. This is in addition to procedures performed in an outpatient setting as noted in our June 11 article.
What services are included?
- Hip surgery
- Hysterectomy
- Knee surgery
- Spine surgery
How does this increased functionality work?
- Start an initial review request in Authorization Manager. (Log in and go to eTools>Authorization Manager.)
- InterQual will launch if you enter a CPT code for hip, knee, spine, or hysterectomy surgery. (InterQual will not launch if you only enter the diagnosis code.)
- The InterQual criteria will display in a checklist format. Make selections based on the patient’s known symptoms, diagnostic testing, and prior treatments. The authorization will be approved automatically* if:
- Criteria are met
- Members’ eligibility is active
- There are no benefit limits
- There is an active referral on file (when required for managed care members)
If the criteria aren’t met, or the code entered is not associated with these services, the authorization will pend for manual review, and you will be notified. Please attach clinical notes.
Resource
Launch InterQual from Authorization Manager fact sheets
* Federal Employee Program member requests will pend for review. Please complete the InterQual steps in Authorization Manager to speed up the approval process.
MPC_012618-1L-78
This article is for all providers caring for our members, except dentists
A combination of sedentary lifestyles, high rates of obesity, and makeshift home workspaces greatly contribute to the second most common reason for sick visits in U.S. adults – low back pain. There are more than 13 million office visits per year for this condition.
Patients often request imaging or surgery because we live in an “on-demand” society, wanting answers and solutions quickly. Imaging can lead to unnecessary exposure to radiation, is not associated with improved outcomes, and burdens patients with significant yet avoidable costs. The NCQA low back pain HEDIS measure recommends that clinicians should avoid ordering imaging within the first 28 days of the onset of their patient’s diagnosis.

Dr. Jayson Carr, a primary care provider with Beth Israel Deaconess HealthCare says: “I tell folks to try to get some exercise more days than not. Finding something that fits into your lifestyle is important so it will be sustainable.”
Read more of Dr. Carr’s thoughts, and a patient’s inspirational story, here.
Tips for talking to patients about low back pain
When speaking with patients who want imaging, you may want to remind them that low back pain can resolve in a few weeks or less with self-care, such as exercise and stretching. Regular and moderate physical activity can prove to be the best medicine, in addition to:
- Ice and heat
- Maintaining a healthy weight
- Over-the-counter pain relievers (ibuprofen, acetaminophen, medicated back patches)
- Physical therapy or chiropractic care
- Proper posture for sitting, standing, and sleeping
- Yoga or Pilates
Linking back to mental health
As you know, chronic pain can often result in depression and insomnia among patients, which can become consuming and amplify and prolong a painful condition. As a senior medical director at Blue Cross, Greg Harris, MD, MPH, recommends screening for depressive symptoms in patients with chronic pain. From there, you’ll be able to discuss and destigmatize the mental health comorbidities of chronic pain, identify stress triggers, and consider multi-disciplinary treatment.
We understand that some patients may not have the ability to schedule an in-person appointment. For these members, we encourage you to promote telehealth visits to get them started on the road to recovery sooner.
Reference our COVID-19 Public Health Emergency temporary payment policy for details on how to bill for telehealth services.
Reference our COVID-19 Public Health Emergency temporary payment policy for details on how to bill for telehealth services. Log in and click Find a Payment Policy on the right side of your home page. Or, go to Office Resources>Policies & Guidelines>Payment Policies.
Additional options
We also cover several alternative treatments for our members, including acupuncture, fitness and weight loss reimbursements, and discounts for other holistic programs. As always, members can verify their benefits by visiting MyBlue at bluecrossma.org, or by calling Member Service at the number on the back of their ID card.
MPC_082521-1P-1-ART
For dentists caring for our members
We offer Dental Blue patients with certain diagnoses additional oral health benefits to help control the management of their condition and its side effects. Last year, we expanded the list of covered conditions to include stroke and Sjögren’s syndrome. We previously reviewed the incidence of stroke and how oral health plays a role in its management. This article will focus on Sjögren’s syndrome.
Source: https://www.sjogrens.org/understanding-sjogrens/symptoms |
How are Sjögren’s syndrome and oral health linked?
Sjögren’s syndrome occurs when a person’s immune system attacks both the glands that produce tears and the salivary ducts, causing dry eyes and mouth. Since many other conditions may also cause these symptoms, it is hard to tell the exact incidence of Sjögren’s syndrome, but experts estimate that this condition may occur in about 1% of the population. It affects many more women than men and usually—but not always—develops in middle adulthood.
The dry mouth caused by Sjögren’s syndrome can cause difficulty in speaking, tasting food, or swallowing. And because saliva helps protect the teeth and the tissues of the oral cavity, people with Sjögren’s syndrome are at increased risk of tooth decay, oral infections, and a higher risk of oral cancer.
What enhanced benefits do we offer?
Dental members with a diagnosis of Sjögren’s syndrome are eligible for cleanings or periodontal maintenance visits four times a year instead of the usual two. These individuals are also eligible for fluoride treatments four time per year and enhanced pre-diagnostic oral cancer screenings twice per year.
How members can enroll
When we can identify members who have Sjögren’s syndrome through their medical claims, we reach out to enroll them in the Enhanced Dental Benefits program. For dental members with other medical insurance, the patient or the patient’s caregiver can enroll by downloading an application (also in "Resources" below) and working with their health care provider to complete and return the form. Once enrolled, the member will be eligible for all of the benefits mentioned above.
We appreciate the dental care that you provide to all of our members. When you see a Dental Blue member with any condition covered by the Enhanced Dental Benefits program, please encourage them to sign up for these additional benefits to maintain their oral and overall health.
Resources
![]() Enhanced Dental Benefit Enrollment Form
Enhanced Dental Benefit Enrollment Form
![]() Dental Blue 65 Enhanced Dental Benefit Enrollment Form
Dental Blue 65 Enhanced Dental Benefit Enrollment Form
MPC_010821-1K-6
This article is for dentists caring for our members
Dental Blue patients with certain diagnoses are eligible for additional oral health benefits to help control the management of their condition and its side effects. Last year, we expanded the list of covered conditions to include stroke and Sjogren’s Syndrome.

How are stroke and oral health linked?
Stroke is the fourth leading cause of death in the US. A number of studies have found links between non-hemorrhagic stroke and oral health.1 Poor oral health can more than double the likelihood of this type of stroke.2 The reason for this seems to be similar to coronary artery disease where certain bacteria from the mouth make their way into the bloodstream, contributing to the development of blockage on the inner walls of the arteries.3 When this process occurs in the brain, the flow of blood in this area is interrupted, leading to ischemia of the brain cells and the development of stroke symptoms.
Dental members with a stroke diagnosis are eligible for cleanings or periodontal maintenance visits four times a year instead of the normal two. Scaling and root planing are covered at 100% when indicated.
How members can enroll
When we can identify members who have had a stroke, we reach out to enroll them in the Enhanced Dental Benefits program. Your patient or the patient’s caregiver can also self-enroll by downloading the Enhanced Dental Benefits Member Self-enrollment form or Dental Blue 65 Enhanced Dental Benefits Member Self-enrollment form found on this page and working with their health care provider to complete and return the form. Once enrolled, the member will be eligible for all of the benefits mentioned above.
We appreciate the dental care that you provide to all of our members. When you see a Dental Blue member with any condition covered by the Enhanced Dental Benefits program, please encourage them to sign up for these additional benefits to maintain their oral and overall health.
MPC_010821-1K-4-ART
1 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5836263/.
2 Fagundes NCF et al. (2019) ‘Periodontitis As A Risk Factor For Stroke: A Systematic Review And Meta-Analysis’, Vascular Health and Risk Management (August 2019), available at https://doi.org/10.2147/VHRM.S204097.
This article is for dentists and oral surgeons, primary care physicians and clinicians, and cardiologists caring for our members
In February, we focus on matters of the heart by celebrating both Valentine’s day and heart health month. This presents you with the opportunity to talk to your patients about maintaining and improving their heart health through regular dental care.
Links between periodontal disease and heart health are clear
The association is clear between periodontal disease–the most common infectious disease in adults–and the control of diabetes1 and the severity of heart disease.2 In fact, notes researcher Robert H. Shmerling, MD, of Harvard Health Publishing, “study after study has shown that people who have poor oral health (such as gum disease or tooth loss) have higher rates of cardiovascular problems such as heart attack or stroke than people with good oral health.”3
That’s why we offer our members Enhanced Dental Benefits. These benefits provide education and full coverage for certain preventive and periodontal services connected to the total health of individuals with certain health conditions--including coronary artery disease, diabetes, and stroke. Services that members can receive with these benefits may help reduce oral inflammation, which has been linked to the management of heart disease. The benefits are paid at 100 percent and are not subject to deductibles, coinsurance, or calendar year maximums when performed by a participating or preferred dental provider.
Enhanced Dental Benefits reduce barriers to care and reduce costs
By reducing cost barriers to care, these benefits have demonstrated results in improving outcomes for members. Our claims data show measurable cost savings – about $5,000, or 20 percent of total medical cost -- when members with both medical and dental coverage diagnosed with heart disease get preventive or periodontal dental care. We are focused not only on helping our dental members get appropriate services to maximize their oral health, but also in helping members control a risk factor in the management of their overall health.
How to help your patients take advantage of their benefits
We automatically identify and enroll members eligible for Enhanced Dental Benefits if they have both medical and dental coverage through Blue Cross of Massachusetts.
For members who only have medical coverage through us, the patient's medical provider can fill out the Enhanced Dental Benefits Enrollment Form for Dental Blue 65 members or all other members.
Once members are enrolled, their dentist can provide more frequent cleaning, periodontal maintenance, and periodontal scaling to put them on the path to improved heart health.
MPC_010323-1P-4-ART
1. https://ncbi.nlm.nih.gov/pmc/articles/PMC8457155/
This article is for primary care providers caring for our members
Keeping blood pressure under control can help reduce the risk of serious health conditions like stroke and heart disease. Nearly half of adults in the U.S. have high blood pressure and many of them don’t even know it, according to the American Heart Association. Partnering with your patients on blood pressure and discussing the importance of blood pressure monitoring can help them understand how to control it.
With the help of Blue Cross and the Institute for Healthcare Improvement, Atrius Health is taking a thoughtful approach to understanding the reasons behind uncontrolled blood pressure in different races. The team conducted focus groups with clinicians, brainstormed pilot ideas with their population health manager and social work teams, and began doing one-on-one patient interviews.
"We’re using what we learn from our interviews with patients and clinicians to make changes,” said Dr. Elizabeth Molina Ortiz, an internist who specializes in family medicine and head of Atrius Health’s Equity Steering Committee.
Atrius’ innovative strategy includes:
- Offering patients with uncontrolled hypertension a blood pressure cuff at no cost.
- Offering video visits with a clinician to monitor hypertension— instead of an in-person visit— to remove barriers like transportation and time constraints.
- Screening patients with uncontrolled blood pressure to see if there are socioeconomic factors contributing to hypertension that they can address by offering support, such as providing medically tailored meals to those who may not have access to healthy food.
Read more in Coverage, An innovative approach to inequities.
Tips to help your patients with blood pressure control
Here are some steps you can take for patients with high blood pressure:
- Encourage patients to monitor blood pressure at home and share their readings. With your guidance, patients can safely and easily monitor their blood pressure at home.
- Discuss the effects of lifestyle choices on blood pressure. Educate your patients on the relationship between lifestyle choices and high blood pressure, as well as the complications associated with uncontrolled blood pressure.
- Promote medication adherence. Talk to your patients about the importance of taking their medications as prescribed. Consider prescribing single-pill medications, when possible, to improve adherence and lower patient out-of-pocket costs.
Remote monitoring simplifies blood pressure management
Blood pressure readings can be taken remotely during telehealth or phone visits using digital reading devices that allow you to document results in your patients’ charts.
Many of our patients may be eligible to receive digital reading devices at no cost by using their health savings account, or by participating in one of our health management programs. We also work with third-party vendors like Livongo® to provide our members with tools and support to help them manage their blood pressure.
HEDIS®’ measure for blood pressure control
The HEDIS controlling high blood pressure (CPB) measure assesses adults:
- Ages 18–85 with a billed diagnosis of hypertension within the last year, AND
- Whose most recent blood pressure reading is <140/90 mm Hg.
When reporting on the HEDIS blood pressure control measure, it is okay to document the average blood pressure reading, but ranges are not eligible for use.
Blood pressure control programs available to our members
Eligible Federal Employee Program (FEP) members can access cuffs through the Hypertension Management Program. FEP members are automatically enrolled in this program when you submit a claim indicating they have hypertension.
Eligible Medicare Advantage members also have a remote monitoring program for hypertension. You can direct your patient to contact the Member Service phone number on their ID card for more information.
As always, thank you for the care you give to your patients—our members.
HEDIS®' is a registered trademark of the National Committee for Quality Assurance (NCQA).
MPC_060722-1R-1
This article is for primary care providers caring for our members
As the season changes, so may the ability to breathe for your patients with persistent asthma. Help your patient understand their triggers, symptoms, and what actions to take by completing an asthma action plan.
In the U.S., asthma disproportionately affects Black, Hispanic, and Native American people. Health inequities in asthma are caused by structural, social, biological, and behavioral determinants. Equity is possible if we work together.
“We can all take steps to address race and health disparities that contribute to asthma and other illnesses,” says Dr. Aaron Bernstein, co-director of the Center for Climate, Health, and the Global Environment at the Harvard T.H. Chan School of Public Health (Harvard Chan C-CHANGE) and a pediatrician at Boston Children’s Hospital. Read more in our Coverage story, A child’s right to breathe.
How the action plan helps
As you know, an asthma action plan is an important tool for patients diagnosed with asthma. The action plan helps patients understand how to manage worsening asthma symptoms to prevent an acute exacerbation. It also supports caregivers and family members in self-managing asthma symptoms.
Control is the goal
Another benefit of the action plan is that it educates patients on how to manage their asthma by using their controller medication regularly. Long-term controller medication adherence helps patients have fewer and milder asthma attacks.
Talk to your patients to ensure their controller medication is working and that they do not over-rely on rescue inhalers. Schedule follow up appointments with patients who request additional rescue medication to reinforce asthma education and promote controller use for asthma management.
We’ll continue outreach this summer
We often review claims to ensure our members have the best health outcomes. If your patient appears to fill their rescue inhaler more often than their controller medication, we may reach out and ask that you follow up with them.
Thank you
As always, thank you for the care you provide to our members.
Resources for members
MPC_031522-1R-3
This article is for medical providers who care for our members with diabetes, coronary artery disease, oral cancer, pregnancy, stroke, and Sjogren’s syndrome
Our Enhanced Dental Benefits program has improved the overall health of our members with specific health conditions by providing them with additional dental benefits. The program offers eligible members additional cleanings and other dental services with no additional deductibles, coinsurance, or calendar year maximums when they are performed by a participating or preferred dental provider.
Beginning September 1, 2019 on their account renewal, members who have been diagnosed with stroke and Sjogren’s syndrome will be eligible for Enhanced Dental Benefits. Members with both conditions may benefit from additional annual cleanings and dental care.

Dr. Athena Pappas, Tufts University School of Dental Medicine |
As of September 1, members who have the following conditions are eligible for the program:
- coronary artery disease (CAD)
- diabetes
- oral cancer
- pregnancy
- Sjogren’s syndrome (new as of September 1, 2019)
- stroke (new as of September 1, 2019).
This program is designed to help your patients receive services that will maintain their health.
The connection between oral health and overall health is clear. For people with many conditions—including diabetes, heart disease, oral cancer, premature births, Sjogren’s syndrome, and stroke—dental care can improve health and well-being.
- Clinical studies have shown an association between periodontal disease – the most common infectious disease in adults – and the control of diabetes1 and the severity of heart disease.2
- Periodontal disease among pregnant women has been associated with an increased risk of delivering a pre-term, low birth-weight baby.3
- Poor oral health has also been associated with the increased likelihood of certain types of stroke4, and dry mouth can be one of the principal signs of Sjogren’s syndrome 5. Members with both conditions may benefit from additional cleanings and dental care.
| Members who have | Can enroll |
|---|---|
| Medical and dental coverage and a medical claim identifying them as having coronary artery disease, diabetes, oral cancer, a stroke, or Sjogren’s syndrome | When we reach out to tell the member about the additional benefits available to them |
or
|
By having their physician complete an enrollment form to certify that they have a qualifying condition |
MPC_041219-1D
This article is for primary care providers, allergists, and pulmonologists caring for our members
Asthma and allergies can affect anyone, but the impact can vary based on race, ethnicity, and income. You play a crucial role in helping your patients with asthma by making sure they understand their triggers, medications, and treatment plan.
We’re making it easier for patients to access their medications
Tier change: Moving certain inhalers to a lower-cost tier
To help lower our members’ out-of-pocket costs for their inhalers and improve adherence to their controller medication, we’re updating the Blue Cross formulary
1. Starting on July 1, 2024, the single-ingredient corticosteroid inhalers listed in the table below will move to a lower-cost tier.
| Name of medication | Moving to this tier on a 2-tier, 3-tier or 5-tier plan on July 1, 2024 | Moving to this tier on a 4-tier or 6-tier plan on July 1, 2024 |
|---|---|---|
| Fluticasone propionate HFA (44 mcg, 110 mcg, 220 mcg) | Tier 1 | Tier 2 |
|
Fluticasone propionate Diskus (50 mcg, 100 mcg, 250 mcg) |
Tier 1 | Tier 2 |
Removing prior authorization
We’re also updating our medical policy 011: Asthma and Chronic Obstructive Pulmonary Disease effective July 1, 2024 to remove prior authorization for Breyna and other generics of budesonide/formoterol.
This will help to reduce administrative burden for you and offer fast access to these products for our members, particularly in acute situations. These medications will continue to have a quantity limit of two inhalers per 30 days.
How you can improve patient outcomes
- Be sure to create an asthma action plan with your patient so they understand their triggers and the appropriate medication to take.
- Share resources that are culturally appropriate and in the patient's preferred language.
- Practice shared decision making with your patients to better understand their individual care preferences and concerns, while building a stronger patient-provider relationship.
- Carefully explain the difference between controller and reliever medication and discuss why controller adherence is important.
- Prescribe a long-term controller medication and provide patient reminders for refills.
- Limit the number of refills on reliever medications to no more than two. If a member requests additional refills, contact them to ensure they’re taking their controller as prescribed, and that it's working for them.
Code claims to exclude patients from asthma quality measures
Certain comorbid conditions, like COPD and emphysema, can exclude members from the asthma medication ratio measure. Avoid coding asthma if the diagnosis is for an asthma-like symptom. Review the conditions below to see if your patient should be excluded.
Using the exclusion codes can eliminate the need to submit patient medical records during HEDIS record collection, saving your staff time and resources.
| Common exclusion codes include | |
|---|---|
| Condition | ICD-10-CM code |
| Acute respiratory failure | J96.00-J96.02, J96.20-J96.22 |
| Chronic obstructive pulmonary disease (COPD) | J44.0, J44.1, J44.9 |
| Chronic respiratory conditions due to fumes or vapors | J68.4 |
| Cystic fibrosis | E84.0, E84.11, E84.19, E84.8, E84.9 |
| Emphysema | J43.0-J43.2, J43.8, J43.9, J98.2, J98.3 |
| Obstructive chronic bronchitis | 491.20-491.22 (ICD-9-CM) |
| Other emphysema | J98.2-J98.3 |
Note that the list above is not exhaustive, but a sample of diagnosis codes that may be used.
Resources
- Adult Asthma Action Plan (English or Spanish)
- Child Asthma Action Plan (English or Spanish)
- Medical policy 011: Asthma and Chronic Obstructive Pulmonary Disease (will be updated on July 1, 2024 as noted above)
- Medication Lookup tool for providers (Blue Cross Blue Shield of Massachusetts formulary)
1. The Blue Cross formulary is used by commercial members with a medical plan that includes pharmacy benefits and group Medex members with a three-tier pharmacy benefit. For FEP members, these medications are:
- Tier 1 for Blue Standard, Basic, and Focus plans
- Tier 2 for Blue Basic and Standard plans with Medicare Prescription Drug Program (MPDP) pharmacy benefits
- Not covered on FEP Blue Focus plans with MPDP pharmacy benefits
MPC_011024-2P-3
This article is for:
- Cardiologists
- Primary care providers
- Discharge planners at acute care hospitals, rehabilitation hospitals, and skilled nursing facilities
We're expanding both our home telemonitoring program and healthy meals program for eligible Medicare Advantage members with congestive heart failure diagnoses. For a full overview of these programs, please see our previous articles.
- Home telemonitoring program for heart failure patients to expand
- Meals, home telemonitoring available to heart failure patients
What's changing?
| Program | Change details |
|---|---|
|
Home telemonitoring
Program description: |
Southcoast VNA has joined and has started accepting referrals as of March 1, 2020. See below for a full list of all home health care providers participating in this pilot program. |
|
Healthy meals
Program description: |
Medicare Advantage members who don’t live in an area where Community Servings delivers can now get meals delivered via UPS. This provides greater access to this program. |
Home health care contacts for referrals for in-home telemonitoring
| Home health care organization participating in-home telemonitoring program | Contact for referrals |
|---|---|
| BAYADA Home Health Care | Phone: 1-508-778-8100 Fax: 1-508-778-5022 bayada.com |
| VNA Care—VNA Care Network & VNA of Boston | Phone: 1-800-728-1862 Fax: 1-774-778-1007 vnacare.org |
Home Health Foundation, a member of Wellforce, including:
|
Phone: 1-978-552-4444 or 1-800-333-4799 Fax: 1-978-552-4401 (Fax their Express Referral Form) Homehealthfoundation.org |
| Southcoast VNA | Phone: 1-800-698-6877, option 3 Fax: 1-508-973-3241 Website: www.southcoastvna.org |
| These providers have a single contact for referrals | |
| Brockton VNA brocktonvna.org |
Visiting Nurse Associations of New England, Inc. (VNANE) Phone: 1-774-404-2205 Fax: 1-508-480-0055 Email (must be encrypted): bcbs@vnane.org Visiting Nurse Associations of New England, Inc. will contact us about your referral. |
| Community Nurse Home Care, Inc. communitynurse.com |
|
| Community Visiting Nurse Agency, Inc. communityvna.com |
|
| GVNA HealthCare gvnahealthcare.org |
|
| Natick Walpole Visiting Nurse Association, Inc. nwvna.org |
|
| Norwell Visiting Nurse Association, Inc. nvna.org |
|
| Porchlight VNA/Home Care porchlighthomecare.org |
|
| Visiting Nurse Community Health, Inc. thevisitingnurses.com |
|
| VNA of Southern Worcester Co., Inc. vnaswc.org |
|
Healthy meal referrals
- Contact Blue Cross Blue Shield of Massachusetts registered nurse, Kerry Nussbaum, at 1-617-246-4721.
- Fill out the Referral for Health Management Programs & Services form. Check off Medicare Advantage Case Management and note the reason for the referral in the notes section. Please fax to the Medicare Advantage number listed on the form.
Questions?
For questions about Blue Cross Blue Shield of Massachusetts’ program, call Tarcia Davis, RN, BSN, CCM, program manager in our case management department, at 1-617-246-4269.
MPC_051818-1S-4
This article is for:
- Cardiologists
- Primary care providers
- Discharge planners at acute care hospitals, rehabilitation hospitals, and skilled nursing facilities
We’re expanding our home telemonitoring program for eligible Medicare Advantage members with congestive heart failure diagnoses. As of November 1, 2019, the home health care providers listed below will join the program and can accept referrals.
 Home Health Foundation (member of Wellforce), which includes:
Home Health Foundation (member of Wellforce), which includes:
- Circle Home (home health care)
- Hallmark Health Visiting Nurse Association
- Home Health VNA
See below for a full list of all home health care providers participating in this pilot program.
What is home telemonitoring?
Telemonitoring gives the member’s physician important information about their daily vital signs. It also can be used as a tool to educate the member on good nutrition, symptom management, and self-care for their condition.
This program helps members self-manage their condition and may keep them out of the hospital or reduce readmission rates.
Who is eligible?
We also offer a healthy meals program to Medicare Advantage members with CHF that provides medically tailored, nutritional meals. Read more.
Medicare Advantage members may be eligible to receive this service through their home health care benefit. They do not need to be homebound to participate. In addition, the member must:
- Have a congestive heart failure (CHF) diagnosis.
- Benefit from having their vital signs monitored (blood pressure, pulse pressure, pulse oxygen, weight).
There’s no additional cost to the member if they meet the program criteria.
How does it work?
Once we identify a member (or receive a referral from the member’s provider), Blue Cross Blue Shield of Massachusetts works with the home health care provider.
The home health care provider will contact the member’s primary care provider to get an order for the services and the acceptable ranges for monitored vital signs.
Then, the home health care provider goes to the member’s home to complete an initial assessment. During their in-home visit, the registered nurse will assess whether the member is physically and cognitively appropriate for telemonitoring and provide any educational needs they may have. The registered nurse can also assess other unmet needs, such as meals and transportation, and suggest resources.
If the member meets assessment criteria, the nurse will install the equipment and show the member how to use it.
Telemonitoring typically lasts six to eight weeks. When the member is discharged, the primary care provider is notified with a detailed discharge summary. If applicable, Blue Cross case managers will continue to follow the member by phone with periodic check-ins.
Home health care contacts for referrals
| Participating providers | Contact for referrals |
|---|---|
| BAYADA Home Health Care |
|
| VNA Care—VNA Care Network & VNA of Boston |
|
Home Health Foundation, a member of Wellforce, including:
|
|
| These providers have a single contact for referrals | |
| Brockton VNA brocktonvna.org |
Visiting Nurse Associations of New England, Inc. (VNANE)
Visiting Nurse Associations of New England, Inc. will contact us about your referral. |
| Community Nurse Home Care, Inc. communitynurse.com |
|
| Community Visiting Nurse Agency, Inc. communityvna.com |
|
| GVNA HealthCare gvnahealthcare.org |
|
| Natick Walpole Visiting Nurse Association, Inc. nwvna.org |
|
| Norwell Visiting Nurse Association, Inc. nvna.org |
|
| Porchlight VNA/Home Care porchlighthomecare.org |
|
| Visiting Nurse Community Health, Inc. thevisitingnurses.com |
|
| VNA of Southern Worcester Co., Inc. vnaswc.org |
|
Questions?
For questions about Blue Cross Blue Shield of Massachusetts’ program, call Tarcia Davis, RN, BSN, CCM, program manager in our case management department, at 1-617-246-4269.
MPC_051818-1S-3

Read more of Dr. Dallow’s thoughts on how COVID-19 changed telehealth in this USA Today article: The pandemic ushered in a 'new era of medicine': These telehealth trends are likely here to stay. |
This article is for all providers caring for our members
The use of telehealth as a site of service has skyrocketed as a result of the COVID-19 pandemic. Before the pandemic, Blue Cross typically received 200 telehealth claims per day. Now we get about 30,000 per day.
This major uptick can be attributed mainly to mental health and primary care.
- Mental health appointments make up 53% of the total telehealth claims processed since March 2020.
- Primary care comprised the second largest percentage of health care appointments at 17%1.
“The flexibility of telehealth has allowed doctors to organize their workday to cater to both in-person and virtual appointments,” says Dr. Katherine Dallow, Blue Cross vice president of clinical programs and strategy. “This means fewer people in the office at one time, creating more opportunities for social distancing.”
1. The pandemic ushered in a 'new era of medicine': These telehealth trends are likely here to stay,” Rodriguez, Adrianna, USA Today, March 21, 2021, retrieved April 7, 2021.
MPC_030620-1N-183
This article is for medical and dental providers caring for our youngest members
A clinical recommendation is the number one reason parents choose to vaccinate their child against HPV. Starting patients on their HPV vaccine when they’re between ages 9-12 can help complete the vaccine schedule sooner, by only requiring two doses—rather than three later in life.
What to say to patients and parents
- Administer all recommended vaccines: Now that your son is 10, he is due for vaccinations to help protect him from meningitis, HPV cancers, and whooping cough.
- Address the risks: HPV is a very common infection in teens and adults. Nearly everyone will get HPV at some point in their lives. Starting the vaccination series today will help protect your child from the cancers and diseases caused by HPV later in their lives.
- Address parent concerns: Studies show that getting vaccinated doesn’t make kids more likely to start having sex. Vaccines protect your child before they are exposed to an infection. That’s why we give HPV vaccination earlier rather than later, to protect them long before they are ever exposed.
Talk to your patient and their parents about the HPV vaccine, and you could help prevent more than 90% of cancers that are caused by HPV.
Steps you can take
- Administer all recommended vaccines during routine visits to streamline scheduling.
- Know your vaccination rates. Monitor patients who are overdue for vaccines and learn why they might be.
- Acknowledge parents’ concerns and be sure to address them specifically.
- Advise parents on conflicting information and help them understand that the HPV vaccine is effective and helps prevent cancer.
Documentation details for HEDIS®
The Immunizations for Adolescents (IMA) measure assesses the percentage of 13-year-old adolescent members who have had:
- Two or three doses of human papillomavirus (HPV) vaccine between the member’s 9th and 13th birthdays.
Documentation must include the vaccination date(s) with at least one of the following:
- Certificate of immunization
- Progress notes
- Date of encounter must be on or before the 13th birthday
- Diagnostic report
- Problem list
|
|
|
|---|---|
| HPV | 90649, 90650, 90651 |
Resources
- Coverage: ‘Why wouldn’t we all want to protect our children against a preventable disease?’
- HPV fact sheet for members
- HPV Coalition Dental Toolkits
HEDIS® is a registered trademark of the National Committee for Quality Assurance (NCQA).
MPC_072022-2I-1
This article is for all providers who provide vaccines to our members

“Because of COVID-19, everything has fallen behind,” said Dr. Simone Wildes, an infectious disease specialist at South Shore Health. She noted a federal report that found first and second doses of measles, mumps, and rubella vaccine – also called MMR – fell 22% and 63%, respectively, in 2020.
Read more in Coverage: Is your child up to date on their shots?
Did you know that a clinical recommendation from a health care provider is the number one reason that patients get vaccinated? Encourage your patients to keep their vaccinations up to date.
We’re sending reminders to members
We want you to know that we’re encouraging our members—your patients—to reach out to you if they aren’t current with their vaccines. This month, we’re sending emails and texts to the parents or guardians of the following members, with these recommendations:
| Age group | Should receive |
|---|---|
|
Children |
All should be received by their second birthday. |
|
Adolescents |
All should be received by the thirteenth birthday. |
We’re sending reminders to members
We want you to know that we’re encouraging our members—your patients—to reach out to you if they aren’t current with their vaccines. This month, we’re sending emails and texts to the parents or guardians of the following members, with these recommendations:
MPC_072022-2I-2
This article is for billing agencies and office staff who bill outpatient cancer treatments

To help your outpatient oncology claims process seamlessly, we’d like to remind you to bill the appropriate cancer diagnosis (not medical diagnosis) in the primary position on your claims. This will help you avoid submitting a replacement claim or sending in an appeal.
Billing in this way helps us process the claim against the member’s benefits so we can apply the member’s appropriate liability based on their plan.
As always, thank you for the cancer care you provide to our members.
MPC_011819-1U-24
This article is for providers ordering high-technology radiology services
We have noticed an increase in appeals for denied authorizations for high-technology radiology services that subsequently were overturned when the provider submitted clinical documentation. To both minimize denials that require your office to spend time submitting appeals and help your patients get the appropriate care sooner, we’ve assembled a few tips.
Tips
- Carelon Medical Benefits Management, an independent company, manages several authorization programs on our behalf. Enter authorization requests using their secure ProviderPortal. It’s available when you log in to Provider Central.
- When a request requires further clinical review, a pop-up window asking for Additional Information will display, as shown below. Please add any other relevant information to the request and click Continue. Include relevant clinical information such as the results of previous studies (for example, labs, X-rays) and treatments, including their duration.
- Make sure you have pop-up blockers turned off since ProviderPortal uses pop-up boxes to prompt you through the system.
For more information about our authorization program, consult the high-technology radiology page on Provider Central.
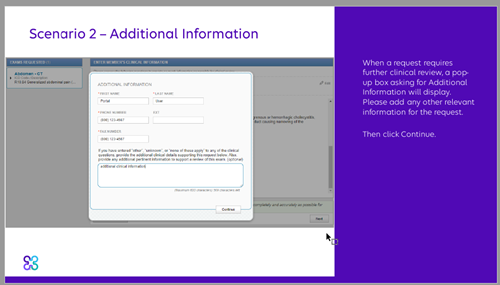
MPC_110223-1R-1
This article is for all providers caring for our members
 We have an important message for our members: Mental health is as important as physical health. That’s why on November 9 we’re launching an advertising campaign and a new online mental health resource center that spotlights mental health resources and care options aimed at reducing stigma around this very important topic.
We have an important message for our members: Mental health is as important as physical health. That’s why on November 9 we’re launching an advertising campaign and a new online mental health resource center that spotlights mental health resources and care options aimed at reducing stigma around this very important topic.
The mental health resource center is designed to help members better understand their mental health care options and explore timely articles and content. With easy access from our public website, our goal is to encourage members to explore and use their mental health resources.
"We are committed to supporting our members in finding the right mental health care—especially important now when they may be feeling overwhelmed and unsure about how to address their mental health needs,” said Ken Duckworth, Senior Medical Director of Behavioral Health.
"This resource center will support our members at a time when access to high-quality mental health services has never been more important,” he said.
1-888-389-7764.
- Remote therapy visits (with costs waived during the Massachusetts health emergency*)
- Self-guided programs
- Wellness offerings
- Substance use support
*Exceptions: Medicare Advantage members will have a cost share for telehealth services. The Federal Employee Program (FEP) is following guidelines from the Blue Cross Blue Shield Association regarding coverage for FEP members for the duration of the state of emergency. For more details see fepblue.org.
- How to help a loved one struggling with mental health
- Talking to kids about COVID-19
- Racial disparity and mental health
- Anxiety and depression in college, among many other relevant issues
The Mental Health Resource Center offers quick access to their specific plan benefit information and the ability to search for a therapist or other mental health provider if they need to.
If members can’t find the information they need or understand their benefits, Team Blue is just a phone call away at 1-888-389-7764. Our service representatives are dedicated to helping members find the care they need and can connect members to a health care expert if needed.
No segment of the population is immune from the effect of COVID-19. And how each person addresses individual mental health concerns and stresses varies dramatically. To address these issues, we are sponsoring a virtual event in partnership with the Boston Globe on November 12: "Navigating the Complexities of Mental Health Amidst a Pandemic."
A panel of mental health specialists will address the complexities of treating mental health during this pandemic.
| When | Thursday, November 12, Noon – 1:00 p.m. |
|---|---|
| Speakers |
|
| Panelists |
|
MPC_092520-1G-2
Blue Cross is dedicated to developing and executing quality initiatives in partnership with our providers. We want you to know that the following information is available on our website.
| Programs & guidelines | To learn more, go to |
|---|---|
| Health management programs Resources about case management, care management for chronic conditions, and referrals. |
Health Management Programs |
| Medical necessity We use Change Healthcare’s criteria as well as supplemental guidelines to determine medical necessity. |
InterQual® Criteria & SmartSheets
Coverage Criteria & Guidelines (for certain services that are not addressed by InterQual criteria or medical policies)
|
| Medical policies Medical policies will help you to determine what we cover and why. |
Medical Policies |
| Member rights and responsibilities Information about access-to-care and member rights and responsibilities. |
See Member Rights and Responsibilities by logging in and going to Office Resources>Policies & Guidelines> Provider Manuals. |
About our utilization management standards
As part of our compliance with NCQA, we want providers to understand our standards for utilization management.
- We encourage appropriate use and discourage over- and under-use of health care services.
- We do not reward or offer financial incentives to utilization management staff to encourage decisions that result in under-utilization of care.
- We do not specifically reward practitioners or other individuals for issuing denials of coverage.
- We do not incentivize or encourage barriers to care and service.
- Utilization management decision-making is based only on appropriateness of care and service and existence of coverage.
MPC_011520-1H-1
This article is for providers performing surgical services for our members
 On January 1, 2024, we’ll update and post our Inpatient Only List. This list contains codes for services that Blue Cross only pays for when care takes place on an inpatient basis for our commercial members. We are not changing authorization requirements and you can still use Authorization Manager to check if authorization is required.
On January 1, 2024, we’ll update and post our Inpatient Only List. This list contains codes for services that Blue Cross only pays for when care takes place on an inpatient basis for our commercial members. We are not changing authorization requirements and you can still use Authorization Manager to check if authorization is required.
For Medicare Advantage members, please continue to refer to CMS’ inpatient only list.
MPC_081822-1Y-4
This article is for providers performing surgical services for our members
On January 1, 2023, our Inpatient Only List will take effect. This list contains codes for services that Blue Cross Blue Shield of Massachusetts only pays when care takes place on an inpatient basis for our commercial members. We are not changing authorization requirements and you can still use Authorization Manager to check if authorization is required.
The Inpatient Only list will replace the Outpatient & Surgical Day Care list currently on the Prior Auth Overview page. This change aligns with CMS.
For Medicare Advantage members, please continue to refer to CMS’ inpatient only list.
MPC_081822-1Y-1
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in January 2020 are now available.
In the middle of the medical policy page you will find summaries of Medical and Pharmacy Policy Updates grouped by the month in which the policy or update is effective. Each month’s list is organized alphabetically by policy title. Click on the policy title to view a summary of the update.
FEP Medical Policies Online
To view Federal Employee Program Medical Policies, visit fepblue.org and search for Medical Policies.
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in January 2021 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in January 2022 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in January 2023 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
Lists of new, revised, and clarified medical policies and pharmacy medical policies effective in January 2024 are now available.
Summaries of medical and pharmacy policy updates are listed on the Policy Updates & Feedback page of our medical policy website. Each month’s summary is organized in sections for medical and pharmacy policies that are new, revised, clarified, or retired.
Medicare Advantage policies
For members enrolled in our Medicare Advantage plans, we are required to make coverage determinations for services through the CMS National Coverage Determination (NCD) policies and benefit manuals. In addition, we follow Local Coverage Determination (LCD) policies established by the Massachusetts Medicare Administrative Contractors. When there is no NCD or LCD, we follow our commercial medical policies for Medicare Advantage members. Refer to medical policy 132, Medicare Advantage Management, for a directory of commercial and Medicare policies or to the Medicare Advantage section of our medical policy site.
FEP medical policies
To view Federal Employee Program medical policies, visit fepblue.org and search for Medical Policies.
MPC_110215-3D
- Providers who order outpatient cancer treatment for our members and their office staff
- Servicing providers for outpatient cancer treatments and their office staff
 As a reminder, starting July 1, 2021, outpatient cancer care will require authorization for commercial and Medicare Advantage members. This will be administered by our vendor, AIM Specialty Health®′, through our Quality Care Cancer Program. To help you prepare for this program, we’re hosting a series of webinars that are designed for providers and for office staff who will be requesting authorization.
As a reminder, starting July 1, 2021, outpatient cancer care will require authorization for commercial and Medicare Advantage members. This will be administered by our vendor, AIM Specialty Health®′, through our Quality Care Cancer Program. To help you prepare for this program, we’re hosting a series of webinars that are designed for providers and for office staff who will be requesting authorization.
We have scheduled separate webinars for medical oncology services and radiation oncology services. At the webinar you’ll learn:
- How the program and authorization request processes work
- Which members and services will require authorization
- About S-code reimbursement
- How to use the AIM ProviderPortalSM to enter requests (demo of the tool)
- How to enter authorizations for members receiving cancer treatment before July 1 and who need to continue their care
We’ll also provide you with additional resources and leave time for questions.
Register for the webinars
Please register for a session so we know how many will attend. We’ll need the attendee name, email, and information about your practice or organization, such as NPI. The person registering will receive a confirmation with a calendar invite that can be forwarded.
How to access the webinars
To join by web, click the Meeting link for each session you’d like to attend. Or, join via phone. When you register for the webinar, we’ll also send you a calendar invite with the link. If you are registering others at your practice, please forward the invite to them.
| May | June | July | |
|---|---|---|---|
| Medical oncology |
Thursday, May 13, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
Wednesday, June 9, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
Thursday, July 8, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
|
Thursday, June 24, 2021, 10 a.m. – 11 a.m. Meeting link Join by phone: Meeting number Meeting password: |
|||
| Radiation oncology |
Thursday, May 20, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
Thursday, June 10, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
Thursday, July 15, 2021, noon – 1 p.m. Meeting link Join by phone: Meeting number Meeting password: |
Can’t attend? Here are some helpful resources
- A recording of the webinar will be posted at a later date (available by logging in only)
- A News Alert detailing the program:
Log in and go to News>Current News. Look for this headline under the March 1, 2021 date: Outpatient cancer care requires authorization starting July 1.
As always, thank you for the care you provide to your patients—our members.
MPC_011819-1U-14


